Bela Patel, Amy A. Kirkwood, Clare J. Rowntree, Krisztina Z. Alapi, Emilio Barretta, Laura Clifton-Hadley, Tom Creasey, SooWah Lee, David I. Marks, Anthony V. Moorman, Nicholas Morley, Pip Patrick, Zaynab Rana, Anita Rijneveld, John A. Snowden, Adele K. Fielding
{"title":"针对老年急性淋巴细胞白血病未治疗患者的 2 期研究 UKALL60+ 的结果","authors":"Bela Patel, Amy A. Kirkwood, Clare J. Rowntree, Krisztina Z. Alapi, Emilio Barretta, Laura Clifton-Hadley, Tom Creasey, SooWah Lee, David I. Marks, Anthony V. Moorman, Nicholas Morley, Pip Patrick, Zaynab Rana, Anita Rijneveld, John A. Snowden, Adele K. Fielding","doi":"10.1002/hem3.88","DOIUrl":null,"url":null,"abstract":"<p>Poor outcome for older patients with ALL has multiple attributions, including a higher incidence of high-risk genetic features,<span><sup>1</sup></span> and comorbidities as well as treatment intolerance.<span><sup>2, 3</sup></span> The phase 2 clinical trial UKALL60+ (NCT01616238) was a collaboration between the UK National Cancer Research Institute Adult ALL Group and the Haemato-Oncology Foundation for Adults in the Netherlands (HOVON) to study treatment choices, quality of life (QoL) and outcomes in older patients with ALL. UKALL60+ offered four treatment “pathways”: pathway A for <i>BCR::ABL1</i>+ ALL and pathways B, C, and D offering three choices of intensity for <i>BCR::ABL1</i> negative ALL (Intensive, Intensive-plus and Non-Intensive, respectively), to be selected by investigator and patients. A registration-only choice (Pathway E) was also available. Details of treatment regimens are given in Figure S1. There were no exclusions for any comorbidities. The primary endpoint was complete remission (CR) after a 2-phase induction. Secondary endpoints included event-free survival (EFS) and overall survival (OS), the predictive value of MRD (Ig/TCR quantification, EuroMRD criteria),<span><sup>4</sup></span> patient-reported outcomes, and the relationship between the baseline characteristics (Charlson index. ECOG, Karnofsky and Chemotherapy Risk Assessment Scale for High-Age Patients [CRASH] scores) and treatment option chosen.</p><p>Between January 2013 and November 2018, 121 eligible patients, median age 69 (interquartile range [IQR]: 65–73, range: 55–83), of whom 107 had B-ALL and 14 T-ALL, were recruited at 34 sites (Table S1). Baseline characteristics are shown in Table 1 alongside the characteristics of the 65 patients aged over 60 years that were recruited to the contemporaneous UKALL14 trial, age 25–65 years. A consort diagram is shown in Figure S2.</p><p>Fifty-one of 81 (63%) patients with <i>BCR::ABL1</i> negative disease were allocated to pathway B, 11% (9/81) to pathway C, and the remaining 26% (21/81) to pathway D. At a median follow-up: 65.9 months (IQR: 38.1–80.9), CR rate after two phases of induction, was achieved by 92% (70% confidence interval [CI]: 82.1–97.2) on pathway A, 70.6% (70% CI: 62.6–77.6) on pathway B, 55.6% (70% CI: 33.6–75.9) on pathway C and 47.6% (70% CI: 34.5%–61%) of those on pathway D. No participant achieved CR on study later than end of induction. Molecular remission occurred in 5/25 (20%; A), 13/51 (25.5%; B), 2/9 (22.2%; C), and 1/21 (4.8%; D) with data available. Only 26/121 (21.5%) patients achieved molecular remission at any point. The relationship between MRD and outcome at the three study timepoints is given in Table S2.</p><p>Ninety-six deaths were reported; 32 patients died without achieving CR (22/32, primary cause, ALL). Fifty-six patients died after relapse and eight died in CR (four from infection, three from second malignancies [small cell lung cancer, AML, and CMML] and one unknown). Survival data are shown in Table 1, with the corresponding Kaplan–Meier survival curves in Figure 1. At a median follow-up of 65.9 months (IQR: 38.1–80.9), the estimated 1-year EFS rates were: pathway A: 56.0% (95% CI: 34.8–72.7), pathway B: 54.9% (95% CI: 40.3–67.3), pathway C: 55.6% (95% CI: 20.4–80.5) and pathway D: 25.2% (95% CI: 9.2–45.1). The corresponding OS was: pathway A: 71.4% (95% CI: 49.2−85.2), pathway B: 64.7% (95% CI: 50.0–76.1), pathway C: 53.3% (95% CI: 17.7–79.6), and pathway D: 15.1% (95% CI: 3.8–33.6). The higher initial CR rate for patients with <i>BCR::ABL positive</i> ALL (pathway A) did not result in a markedly better 1-year EFS or OS than the <i>BCR::ABL1</i> negative participants, regardless of pathway. The 3-year EFS (95% CI) were: pathway A: 27.0% (11.5–45.3), pathway B: 16.5% (7.7–28.3), pathway C: 41.7% (10.9–70.8), and pathway D: 15.1% (3.8–33.70) and OS (95% CI): pathway A: 33.0% (15.5–51.8), pathway B: 20.8% (10.8–33.0), pathway C: 55.3% (17.7–79.6) and pathway D: 15.1% (3.8–33.6). Three-year EFS for those achieving CR was 27.6% (18.2–37.8) and for those achieving molecular remission was 33.6% (16.4–51.7), as shown in Figure S3. Only 14 patients with T-ALL were recruited, with no discernable difference in outcome to B-ALL (Table S3). A description of the pathway E, registration-only cohort is given in the supplement.</p><p>Adverse events (AEs), duration of hospitalization, treatment cessation by phase of therapy, are shown in Tables S4 and S5. Five of 121 (4.1%) patients (none of whom had achieved CR) suffered a fatal AE (three pathway C and one each pathways B and D), the causes being one cardiac arrest, three lung infections, and one febrile neutropenia. Grade 3/4 events were common (98/102; 96%), particularly infections (88/102; 86.3%). Patients in pathway C experienced significantly more grade 3/4 AEs during induction 1 (medians 16.0 [IQR: 8.0–20.5]) and induction 2 (15.0 [9.0–17.5]) compared to patients in pathways A (9.0 [6.0–11.0], <i>p</i> = 0.045 [induction 1] and 6.0 [3.0–8.0], <i>p</i> = 0.030 [induction 2]) and D (6.5 [5.5–10.0], <i>p</i> = 0.026 [induction 1] and 5.5 [3.5–8.5], <i>p</i> = 0.026 [induction 2]). More events were also seen for pathway B (10.0 [8.0–13.0], <i>p</i> = 0.023) than pathway D. Only 21/106 (19.8%) patients completed all protocol treatment. Discontinuation was highest during inductions 1 and 2; 27/106 (25.5%) and 11/106 (10.4%) mainly due to refractory/relapsed disease (19/38; 50%). Relapsed/refractory ALL was also the main reason for discontinuation of therapy at other timepoints (33/47; 70.2%) across all arms. Only five of 106 (4.7%) overtly stopped therapy due to toxicity.</p><p>A comparison of patient characteristics across the pathways is shown in Table 1. Participants on pathway D were significantly older than those on pathway B (median 73 years [IQR: 70–78] vs. 67 [IQR: 62–70], <i>p</i> = 0.0001), and had greater comorbidity; 9/21 (45%) with a Charleston Index of 7 or more in pathway D compared to only 8/51 (16.7%) in pathway B. The greater frailty of the pathway D group was also evident when comparing baseline QoL measures and comorbidities, with significantly lower physical functioning compared to pathway B; medians 60.0 (IQR: 53.3–80) versus 86.7 (IQR: 66.7–100), <i>p</i> = 0.014 (Tables S6 and S7). No patient with a Charleston index score of 7 or above was allocated to pathway C (<i>p</i> = 0.013). Major, age-associated comorbidities were common across the entire study cohort and included cardiac disease 27/121 (22.3%), diabetes 17/121 (14.0%), hypertension 39/121 (32.2%), and other cancer 22/121 (18.1%), eight of which were previous breast cancer and seven previous hematological malignancy.</p><p>Significant differences were seen in duration of inpatient stay, analysed by percentage of total treatment period spent in hospital (<i>p</i> = 0.026). Patients receiving pathways B and C spent more treatment-time in hospital compared to pathways A and D, with the effect most pronounced during induction (<i>p</i> = 0.0001) where pathway B and C participants were inpatients for 62.1% (46.3–96.7) and 75.8% (68.8–83.0), respectively compared to pathway A and D participants at 22.8% (IQR: 9.8–55.6) and 31.1% (IQR: 14.5–51.5), respectively. QoL was compared by pathway—summarized in supplementary results. We saw no indication that the least intensive pathway D provided a better QoL, with scores for some scales numerically lower than those of pathways A–C (Figure S4A–D). Any decreases in QoL from baseline were generally seen at the end of induction phases, with improvements in the FACT scores seen by the end of consolidation 1 and maintenance 1 (Table S8). Physical function scores, as assessed by QLQ-C30, remained reduced throughout while sensory and motor neuropathy scores increased at later points during therapy.</p><p>We compared the EFS and OS of UKALL60+ cohort with that of the 65 patients aged 60–65 years, treated on the full intensity adult ALL trial UKALL14 in an overlapping recruitment timeframe. Unsurprisingly, patients in UKALL14 had lower ECOG scores (40.0% vs. 60.9% ECOG 0, <i>p</i> = 0.0068). Fewer had baseline comorbidities (67.7% vs. 85.0%, <i>p</i> = 0.0059)—particularly notable for cardiac morbidities (6.2% vs. 22.5% <i>p</i> = 0.0046). Although CR rates were higher; UKALL14 55/63 (87.3%) vs. UKALL60+ 82/118 (69.2%), as shown in Table 1, EFS and OS rates at 3 years were 20.5% (11.5–31.3) and 25.2% (15.2–36.5) for UKALL14 and 18.8% (12.2–26.5) and 23.2% (15.9–31.4) for UKALL60+ (Figure 1C,D). However, the type of events differed, with only 18/55 (32.7%) being relapse, 9/55 deaths without remission, and 26/55 (47.2%) deaths in remission in UKALL14 compared to 56/95 (58.9%), 32/95 (33.7%), and 7/95 (7.4%) respectively, for UKALL60+. Among the UKALL14 60–65 year-old cohort, 28/65 had received allo-SCT, resulting in death in remission in 3/28 (46%).<span><sup>5</sup></span> Among patients treated on pathway B, there was no difference in outcome between patients with high/very high-risk versus standard-risk genetics (EFS HR: 1.35 [0.68–2.67], <i>p</i> = 0.39) whereas there was a difference in outcome by genetic risk for patients aged 60–65 years old treated on UKALL14 (HR: 2.59 [1.12–5.98], <i>p</i> = 0.026).</p><p>Our survival data are broadly commensurate with data from a GMALL cohort of similar median age<span><sup>6</sup></span> where OS at 3 years was 32%. However, the UKALL60+ population were in worse health overall; 27.5% had a Charlson Index >7 compared to the GMALL cohort, with only 11% scoring >3, commensurate with the GMALL exclusion criteria for comorbidities. By contrast to the GMALL early death rate of 14%, we observed a low treatment-related mortality. UKALL60+ treatments were successfully planned to minimize harm, but this did not improve OS.</p><p>It was unexpected that the 3-year EFS and OS of 20.5% and 25.2% for those aged 60–65 years treated on UKALL14 data did not differ from that of the UKALL60+ recruits, with completely overlapping survival curves (Figure 1). The outcomes are similar to those reported in an EBMT study of 418 patients aged over 55 years receiving alloSCT; 5-year LFS of 34% but a 51% nonrelapse mortality.<span><sup>7</sup></span> Taken together, these data suggest even the most intensive treatments including alloSCT do not generate excellent outcomes for most older patients with ALL. We were surprised to see no evidence of better QoL for the recipients of the least intensive pathway D, despite a significant reduction in length of hospital stay.</p><p>In summary, the UKALL60+ pathways proved safe for initial cytoreduction, but the survival outcomes in this representative population of older patients with ALL was unsatisfactory. Nonchemotherapy approaches should be employed at the earliest opportunity for this patient group. QoL should always be measured, as the investigators assumptions do not necessarily reflect patients' experience.</p><p><b>Bela Patel</b>: Trial design, trial management group member, manuscript writing. <b>Amy A. Kirkwood</b>: Trial design, lead statistician, data analysis, manuscript writing. <b>Clare J. Rowntree</b>: Trial management group member, site principal investigator. <b>Krisztina Z. Alapi</b>: Central lab manager, specimen processing, MRD analysis. <b>Emilio Barretta</b>: Central analysis of genetics. <b>Laura Clifton-Hadley</b>: Trial management group member, lead trial co-ordination. <b>Tom Creasey</b>: Central analysis of genetics. <b>SooWah Lee</b>: Specimen processing, MRD analysis. <b>David I. Marks</b>: Trial management group member, site principal investigator. <b>Anthony V. Moorman</b>: Trial management group member, central coordination of genetics. <b>Nicholas Morley</b>: Trial management group member, site principal investigator. <b>Pip Patrick</b>: Trial management group member, senior trial coordination. <b>Zaynab Rana</b>: Trial management group member, trial coordination. <b>Anita Rijneveld</b>: Site principal investigator, lead for HOVON. <b>John A. Snowden</b>: Trial management group member, quality of life lead. <b>Adele K. Fielding</b>: Trial concept and design, trial management group chair, trial chief investigator, manuscript writing, trial funding.</p><p>The authors declare no conflict of interest.</p><p>Cancer Research UK CRUK/A13920 to AKF, CRUK/A21019 to AKF/AVM, and an unrestricted educational support grant from Jazz Pharma.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 6","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.88","citationCount":"0","resultStr":"{\"title\":\"Results from UKALL60+, a phase 2 study in older patients with untreated acute lymphoblastic leukemia\",\"authors\":\"Bela Patel, Amy A. Kirkwood, Clare J. Rowntree, Krisztina Z. Alapi, Emilio Barretta, Laura Clifton-Hadley, Tom Creasey, SooWah Lee, David I. Marks, Anthony V. Moorman, Nicholas Morley, Pip Patrick, Zaynab Rana, Anita Rijneveld, John A. Snowden, Adele K. Fielding\",\"doi\":\"10.1002/hem3.88\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Poor outcome for older patients with ALL has multiple attributions, including a higher incidence of high-risk genetic features,<span><sup>1</sup></span> and comorbidities as well as treatment intolerance.<span><sup>2, 3</sup></span> The phase 2 clinical trial UKALL60+ (NCT01616238) was a collaboration between the UK National Cancer Research Institute Adult ALL Group and the Haemato-Oncology Foundation for Adults in the Netherlands (HOVON) to study treatment choices, quality of life (QoL) and outcomes in older patients with ALL. UKALL60+ offered four treatment “pathways”: pathway A for <i>BCR::ABL1</i>+ ALL and pathways B, C, and D offering three choices of intensity for <i>BCR::ABL1</i> negative ALL (Intensive, Intensive-plus and Non-Intensive, respectively), to be selected by investigator and patients. A registration-only choice (Pathway E) was also available. Details of treatment regimens are given in Figure S1. There were no exclusions for any comorbidities. The primary endpoint was complete remission (CR) after a 2-phase induction. Secondary endpoints included event-free survival (EFS) and overall survival (OS), the predictive value of MRD (Ig/TCR quantification, EuroMRD criteria),<span><sup>4</sup></span> patient-reported outcomes, and the relationship between the baseline characteristics (Charlson index. ECOG, Karnofsky and Chemotherapy Risk Assessment Scale for High-Age Patients [CRASH] scores) and treatment option chosen.</p><p>Between January 2013 and November 2018, 121 eligible patients, median age 69 (interquartile range [IQR]: 65–73, range: 55–83), of whom 107 had B-ALL and 14 T-ALL, were recruited at 34 sites (Table S1). Baseline characteristics are shown in Table 1 alongside the characteristics of the 65 patients aged over 60 years that were recruited to the contemporaneous UKALL14 trial, age 25–65 years. A consort diagram is shown in Figure S2.</p><p>Fifty-one of 81 (63%) patients with <i>BCR::ABL1</i> negative disease were allocated to pathway B, 11% (9/81) to pathway C, and the remaining 26% (21/81) to pathway D. At a median follow-up: 65.9 months (IQR: 38.1–80.9), CR rate after two phases of induction, was achieved by 92% (70% confidence interval [CI]: 82.1–97.2) on pathway A, 70.6% (70% CI: 62.6–77.6) on pathway B, 55.6% (70% CI: 33.6–75.9) on pathway C and 47.6% (70% CI: 34.5%–61%) of those on pathway D. No participant achieved CR on study later than end of induction. Molecular remission occurred in 5/25 (20%; A), 13/51 (25.5%; B), 2/9 (22.2%; C), and 1/21 (4.8%; D) with data available. Only 26/121 (21.5%) patients achieved molecular remission at any point. The relationship between MRD and outcome at the three study timepoints is given in Table S2.</p><p>Ninety-six deaths were reported; 32 patients died without achieving CR (22/32, primary cause, ALL). Fifty-six patients died after relapse and eight died in CR (four from infection, three from second malignancies [small cell lung cancer, AML, and CMML] and one unknown). Survival data are shown in Table 1, with the corresponding Kaplan–Meier survival curves in Figure 1. At a median follow-up of 65.9 months (IQR: 38.1–80.9), the estimated 1-year EFS rates were: pathway A: 56.0% (95% CI: 34.8–72.7), pathway B: 54.9% (95% CI: 40.3–67.3), pathway C: 55.6% (95% CI: 20.4–80.5) and pathway D: 25.2% (95% CI: 9.2–45.1). The corresponding OS was: pathway A: 71.4% (95% CI: 49.2−85.2), pathway B: 64.7% (95% CI: 50.0–76.1), pathway C: 53.3% (95% CI: 17.7–79.6), and pathway D: 15.1% (95% CI: 3.8–33.6). The higher initial CR rate for patients with <i>BCR::ABL positive</i> ALL (pathway A) did not result in a markedly better 1-year EFS or OS than the <i>BCR::ABL1</i> negative participants, regardless of pathway. The 3-year EFS (95% CI) were: pathway A: 27.0% (11.5–45.3), pathway B: 16.5% (7.7–28.3), pathway C: 41.7% (10.9–70.8), and pathway D: 15.1% (3.8–33.70) and OS (95% CI): pathway A: 33.0% (15.5–51.8), pathway B: 20.8% (10.8–33.0), pathway C: 55.3% (17.7–79.6) and pathway D: 15.1% (3.8–33.6). Three-year EFS for those achieving CR was 27.6% (18.2–37.8) and for those achieving molecular remission was 33.6% (16.4–51.7), as shown in Figure S3. Only 14 patients with T-ALL were recruited, with no discernable difference in outcome to B-ALL (Table S3). A description of the pathway E, registration-only cohort is given in the supplement.</p><p>Adverse events (AEs), duration of hospitalization, treatment cessation by phase of therapy, are shown in Tables S4 and S5. Five of 121 (4.1%) patients (none of whom had achieved CR) suffered a fatal AE (three pathway C and one each pathways B and D), the causes being one cardiac arrest, three lung infections, and one febrile neutropenia. Grade 3/4 events were common (98/102; 96%), particularly infections (88/102; 86.3%). Patients in pathway C experienced significantly more grade 3/4 AEs during induction 1 (medians 16.0 [IQR: 8.0–20.5]) and induction 2 (15.0 [9.0–17.5]) compared to patients in pathways A (9.0 [6.0–11.0], <i>p</i> = 0.045 [induction 1] and 6.0 [3.0–8.0], <i>p</i> = 0.030 [induction 2]) and D (6.5 [5.5–10.0], <i>p</i> = 0.026 [induction 1] and 5.5 [3.5–8.5], <i>p</i> = 0.026 [induction 2]). More events were also seen for pathway B (10.0 [8.0–13.0], <i>p</i> = 0.023) than pathway D. Only 21/106 (19.8%) patients completed all protocol treatment. Discontinuation was highest during inductions 1 and 2; 27/106 (25.5%) and 11/106 (10.4%) mainly due to refractory/relapsed disease (19/38; 50%). Relapsed/refractory ALL was also the main reason for discontinuation of therapy at other timepoints (33/47; 70.2%) across all arms. Only five of 106 (4.7%) overtly stopped therapy due to toxicity.</p><p>A comparison of patient characteristics across the pathways is shown in Table 1. Participants on pathway D were significantly older than those on pathway B (median 73 years [IQR: 70–78] vs. 67 [IQR: 62–70], <i>p</i> = 0.0001), and had greater comorbidity; 9/21 (45%) with a Charleston Index of 7 or more in pathway D compared to only 8/51 (16.7%) in pathway B. The greater frailty of the pathway D group was also evident when comparing baseline QoL measures and comorbidities, with significantly lower physical functioning compared to pathway B; medians 60.0 (IQR: 53.3–80) versus 86.7 (IQR: 66.7–100), <i>p</i> = 0.014 (Tables S6 and S7). No patient with a Charleston index score of 7 or above was allocated to pathway C (<i>p</i> = 0.013). Major, age-associated comorbidities were common across the entire study cohort and included cardiac disease 27/121 (22.3%), diabetes 17/121 (14.0%), hypertension 39/121 (32.2%), and other cancer 22/121 (18.1%), eight of which were previous breast cancer and seven previous hematological malignancy.</p><p>Significant differences were seen in duration of inpatient stay, analysed by percentage of total treatment period spent in hospital (<i>p</i> = 0.026). Patients receiving pathways B and C spent more treatment-time in hospital compared to pathways A and D, with the effect most pronounced during induction (<i>p</i> = 0.0001) where pathway B and C participants were inpatients for 62.1% (46.3–96.7) and 75.8% (68.8–83.0), respectively compared to pathway A and D participants at 22.8% (IQR: 9.8–55.6) and 31.1% (IQR: 14.5–51.5), respectively. QoL was compared by pathway—summarized in supplementary results. We saw no indication that the least intensive pathway D provided a better QoL, with scores for some scales numerically lower than those of pathways A–C (Figure S4A–D). Any decreases in QoL from baseline were generally seen at the end of induction phases, with improvements in the FACT scores seen by the end of consolidation 1 and maintenance 1 (Table S8). Physical function scores, as assessed by QLQ-C30, remained reduced throughout while sensory and motor neuropathy scores increased at later points during therapy.</p><p>We compared the EFS and OS of UKALL60+ cohort with that of the 65 patients aged 60–65 years, treated on the full intensity adult ALL trial UKALL14 in an overlapping recruitment timeframe. Unsurprisingly, patients in UKALL14 had lower ECOG scores (40.0% vs. 60.9% ECOG 0, <i>p</i> = 0.0068). Fewer had baseline comorbidities (67.7% vs. 85.0%, <i>p</i> = 0.0059)—particularly notable for cardiac morbidities (6.2% vs. 22.5% <i>p</i> = 0.0046). Although CR rates were higher; UKALL14 55/63 (87.3%) vs. UKALL60+ 82/118 (69.2%), as shown in Table 1, EFS and OS rates at 3 years were 20.5% (11.5–31.3) and 25.2% (15.2–36.5) for UKALL14 and 18.8% (12.2–26.5) and 23.2% (15.9–31.4) for UKALL60+ (Figure 1C,D). However, the type of events differed, with only 18/55 (32.7%) being relapse, 9/55 deaths without remission, and 26/55 (47.2%) deaths in remission in UKALL14 compared to 56/95 (58.9%), 32/95 (33.7%), and 7/95 (7.4%) respectively, for UKALL60+. Among the UKALL14 60–65 year-old cohort, 28/65 had received allo-SCT, resulting in death in remission in 3/28 (46%).<span><sup>5</sup></span> Among patients treated on pathway B, there was no difference in outcome between patients with high/very high-risk versus standard-risk genetics (EFS HR: 1.35 [0.68–2.67], <i>p</i> = 0.39) whereas there was a difference in outcome by genetic risk for patients aged 60–65 years old treated on UKALL14 (HR: 2.59 [1.12–5.98], <i>p</i> = 0.026).</p><p>Our survival data are broadly commensurate with data from a GMALL cohort of similar median age<span><sup>6</sup></span> where OS at 3 years was 32%. However, the UKALL60+ population were in worse health overall; 27.5% had a Charlson Index >7 compared to the GMALL cohort, with only 11% scoring >3, commensurate with the GMALL exclusion criteria for comorbidities. By contrast to the GMALL early death rate of 14%, we observed a low treatment-related mortality. UKALL60+ treatments were successfully planned to minimize harm, but this did not improve OS.</p><p>It was unexpected that the 3-year EFS and OS of 20.5% and 25.2% for those aged 60–65 years treated on UKALL14 data did not differ from that of the UKALL60+ recruits, with completely overlapping survival curves (Figure 1). The outcomes are similar to those reported in an EBMT study of 418 patients aged over 55 years receiving alloSCT; 5-year LFS of 34% but a 51% nonrelapse mortality.<span><sup>7</sup></span> Taken together, these data suggest even the most intensive treatments including alloSCT do not generate excellent outcomes for most older patients with ALL. We were surprised to see no evidence of better QoL for the recipients of the least intensive pathway D, despite a significant reduction in length of hospital stay.</p><p>In summary, the UKALL60+ pathways proved safe for initial cytoreduction, but the survival outcomes in this representative population of older patients with ALL was unsatisfactory. Nonchemotherapy approaches should be employed at the earliest opportunity for this patient group. QoL should always be measured, as the investigators assumptions do not necessarily reflect patients' experience.</p><p><b>Bela Patel</b>: Trial design, trial management group member, manuscript writing. <b>Amy A. Kirkwood</b>: Trial design, lead statistician, data analysis, manuscript writing. <b>Clare J. Rowntree</b>: Trial management group member, site principal investigator. <b>Krisztina Z. Alapi</b>: Central lab manager, specimen processing, MRD analysis. <b>Emilio Barretta</b>: Central analysis of genetics. <b>Laura Clifton-Hadley</b>: Trial management group member, lead trial co-ordination. <b>Tom Creasey</b>: Central analysis of genetics. <b>SooWah Lee</b>: Specimen processing, MRD analysis. <b>David I. Marks</b>: Trial management group member, site principal investigator. <b>Anthony V. Moorman</b>: Trial management group member, central coordination of genetics. <b>Nicholas Morley</b>: Trial management group member, site principal investigator. <b>Pip Patrick</b>: Trial management group member, senior trial coordination. <b>Zaynab Rana</b>: Trial management group member, trial coordination. <b>Anita Rijneveld</b>: Site principal investigator, lead for HOVON. <b>John A. Snowden</b>: Trial management group member, quality of life lead. <b>Adele K. Fielding</b>: Trial concept and design, trial management group chair, trial chief investigator, manuscript writing, trial funding.</p><p>The authors declare no conflict of interest.</p><p>Cancer Research UK CRUK/A13920 to AKF, CRUK/A21019 to AKF/AVM, and an unrestricted educational support grant from Jazz Pharma.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 6\",\"pages\":\"\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2024-06-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.88\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.88\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.88","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
只有 21/106 例(19.8%)患者完成了所有治疗方案。)只有 21/106 例(19.8%)患者完成了所有方案治疗。在第1和第2次诱导期间,终止治疗的比例最高,分别为27/106(25.5%)和11/106(10.4%),主要是由于难治性/复发性疾病(19/38;50%)。复发/难治性 ALL 也是所有治疗组在其他时间点终止治疗的主要原因(33/47;70.2%)。106例患者中只有5例(4.7%)因毒性明显停止治疗。路径 D 的参与者明显比路径 B 的参与者年长(中位数为 73 岁 [IQR: 70-78] vs. 67 岁 [IQR: 62-70],p = 0.0001),且合并症较多;路径 D 中查尔斯顿指数为 7 或以上的患者有 9/21 人(45%),而路径 B 中仅有 8/51 人(16.7%)。在比较基线 QoL 指标和合并症时,路径 D 组患者更虚弱的情况也很明显,身体功能明显低于路径 B 组;中位数为 60.0(IQR:53.3-80)对 86.7(IQR:66.7-100),p = 0.014(表 S6 和 S7)。没有查尔斯顿指数为 7 分或以上的患者被分配到路径 C(p = 0.013)。与年龄相关的主要合并症在整个研究队列中很常见,包括心脏病 27/121 例(22.3%)、糖尿病 17/121 例(14.0%)、高血压 39/121 例(32.2%)和其他癌症 22/121 例(18.1%),其中 8 例曾患乳腺癌,7 例曾患血液恶性肿瘤。与路径A和路径D相比,接受路径B和路径C的患者住院治疗的时间更长,在诱导期间的影响最为明显(p = 0.0001),路径B和路径C参与者的住院时间分别为62.1%(46.3-96.7)和75.8%(68.8-83.0),而路径A和路径D参与者的住院时间分别为22.8%(IQR:9.8-55.6)和31.1%(IQR:14.5-51.5)。QoL按途径进行了比较--总结见补充结果。没有迹象表明强化程度最低的路径 D 能提供更好的 QoL,某些量表的得分在数值上低于路径 A-C(图 S4A-D)。与基线相比,QoL 的任何下降一般都出现在诱导阶段的末期,而在巩固 1 和维持 1 阶段末期,FACT 分数有所改善(表 S8)。我们将UKALL60+队列的EFS和OS与65名60-65岁患者的EFS和OS进行了比较,这些患者是在招募时间重叠的UKALL14成人ALL试验中接受治疗的。不出所料,UKALL14 的患者 ECOG 评分较低(40.0% 对 60.9% ECOG 0,P = 0.0068)。基线合并症较少(67.7% vs. 85.0%,p = 0.0059),尤其是心脏疾病(6.2% vs. 22.5% p = 0.0046)。虽然 CR 率更高;UKALL14 55/63 (87.3%) vs. UKALL60+ 82/118 (69.2%),如表 1 所示,UKALL14 3 年的 EFS 和 OS 率分别为 20.5% (11.5-31.3) 和 25.2% (15.2-36.5),UKALL60+ 为 18.8% (12.2-26.5) 和 23.2% (15.9-31.4)(图 1C、D)。然而,事件的类型有所不同,UKALL14中只有18/55(32.7%)人复发,9/55人在病情未缓解时死亡,26/55(47.2%)人在病情缓解时死亡,而UKALL60+中分别为56/95(58.9%)、32/95(33.7%)和7/95(7.4%)。在 UKALL14 60-65 岁的队列中,有 28/65 人接受了异体 SCT,结果有 3/28 人(46%)在缓解期死亡。5 在接受路径 B 治疗的患者中,高风险/极高风险遗传学患者与标准风险遗传学患者的预后无差异(EFS HR:1.35 [0.68-2.我们的生存数据与中位年龄相似的 GMALL 队列6 的数据基本一致,后者 3 年的 OS 为 32%。然而,UKALL60+人群的总体健康状况较差;与GMALL队列相比,27.5%的人的Charlson指数为>7,只有11%的人的指数为>3,与GMALL的合并症排除标准相符。与 GMALL 14% 的早期死亡率相比,我们观察到与治疗相关的死亡率很低。UKALL60+的治疗计划成功地将伤害降到了最低,但这并没有改善OS.出乎意料的是,根据UKALL14数据接受治疗的60-65岁患者的3年EFS和OS分别为20.5%和25.2%,与UKALL60+招募者的情况并无不同,生存曲线完全重叠(图1)。这些结果与 EBMT 一项针对 418 名 55 岁以上接受异体干细胞移植患者的研究中报告的结果相似;5 年 LFS 为 34%,但非复发死亡率为 51%。
Results from UKALL60+, a phase 2 study in older patients with untreated acute lymphoblastic leukemia
Poor outcome for older patients with ALL has multiple attributions, including a higher incidence of high-risk genetic features,1 and comorbidities as well as treatment intolerance.2, 3 The phase 2 clinical trial UKALL60+ (NCT01616238) was a collaboration between the UK National Cancer Research Institute Adult ALL Group and the Haemato-Oncology Foundation for Adults in the Netherlands (HOVON) to study treatment choices, quality of life (QoL) and outcomes in older patients with ALL. UKALL60+ offered four treatment “pathways”: pathway A for BCR::ABL1+ ALL and pathways B, C, and D offering three choices of intensity for BCR::ABL1 negative ALL (Intensive, Intensive-plus and Non-Intensive, respectively), to be selected by investigator and patients. A registration-only choice (Pathway E) was also available. Details of treatment regimens are given in Figure S1. There were no exclusions for any comorbidities. The primary endpoint was complete remission (CR) after a 2-phase induction. Secondary endpoints included event-free survival (EFS) and overall survival (OS), the predictive value of MRD (Ig/TCR quantification, EuroMRD criteria),4 patient-reported outcomes, and the relationship between the baseline characteristics (Charlson index. ECOG, Karnofsky and Chemotherapy Risk Assessment Scale for High-Age Patients [CRASH] scores) and treatment option chosen.
Between January 2013 and November 2018, 121 eligible patients, median age 69 (interquartile range [IQR]: 65–73, range: 55–83), of whom 107 had B-ALL and 14 T-ALL, were recruited at 34 sites (Table S1). Baseline characteristics are shown in Table 1 alongside the characteristics of the 65 patients aged over 60 years that were recruited to the contemporaneous UKALL14 trial, age 25–65 years. A consort diagram is shown in Figure S2.
Fifty-one of 81 (63%) patients with BCR::ABL1 negative disease were allocated to pathway B, 11% (9/81) to pathway C, and the remaining 26% (21/81) to pathway D. At a median follow-up: 65.9 months (IQR: 38.1–80.9), CR rate after two phases of induction, was achieved by 92% (70% confidence interval [CI]: 82.1–97.2) on pathway A, 70.6% (70% CI: 62.6–77.6) on pathway B, 55.6% (70% CI: 33.6–75.9) on pathway C and 47.6% (70% CI: 34.5%–61%) of those on pathway D. No participant achieved CR on study later than end of induction. Molecular remission occurred in 5/25 (20%; A), 13/51 (25.5%; B), 2/9 (22.2%; C), and 1/21 (4.8%; D) with data available. Only 26/121 (21.5%) patients achieved molecular remission at any point. The relationship between MRD and outcome at the three study timepoints is given in Table S2.
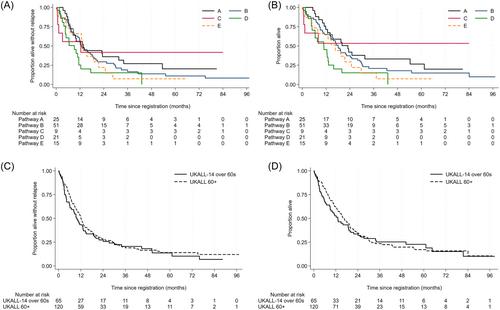
Ninety-six deaths were reported; 32 patients died without achieving CR (22/32, primary cause, ALL). Fifty-six patients died after relapse and eight died in CR (four from infection, three from second malignancies [small cell lung cancer, AML, and CMML] and one unknown). Survival data are shown in Table 1, with the corresponding Kaplan–Meier survival curves in Figure 1. At a median follow-up of 65.9 months (IQR: 38.1–80.9), the estimated 1-year EFS rates were: pathway A: 56.0% (95% CI: 34.8–72.7), pathway B: 54.9% (95% CI: 40.3–67.3), pathway C: 55.6% (95% CI: 20.4–80.5) and pathway D: 25.2% (95% CI: 9.2–45.1). The corresponding OS was: pathway A: 71.4% (95% CI: 49.2−85.2), pathway B: 64.7% (95% CI: 50.0–76.1), pathway C: 53.3% (95% CI: 17.7–79.6), and pathway D: 15.1% (95% CI: 3.8–33.6). The higher initial CR rate for patients with BCR::ABL positive ALL (pathway A) did not result in a markedly better 1-year EFS or OS than the BCR::ABL1 negative participants, regardless of pathway. The 3-year EFS (95% CI) were: pathway A: 27.0% (11.5–45.3), pathway B: 16.5% (7.7–28.3), pathway C: 41.7% (10.9–70.8), and pathway D: 15.1% (3.8–33.70) and OS (95% CI): pathway A: 33.0% (15.5–51.8), pathway B: 20.8% (10.8–33.0), pathway C: 55.3% (17.7–79.6) and pathway D: 15.1% (3.8–33.6). Three-year EFS for those achieving CR was 27.6% (18.2–37.8) and for those achieving molecular remission was 33.6% (16.4–51.7), as shown in Figure S3. Only 14 patients with T-ALL were recruited, with no discernable difference in outcome to B-ALL (Table S3). A description of the pathway E, registration-only cohort is given in the supplement.
Adverse events (AEs), duration of hospitalization, treatment cessation by phase of therapy, are shown in Tables S4 and S5. Five of 121 (4.1%) patients (none of whom had achieved CR) suffered a fatal AE (three pathway C and one each pathways B and D), the causes being one cardiac arrest, three lung infections, and one febrile neutropenia. Grade 3/4 events were common (98/102; 96%), particularly infections (88/102; 86.3%). Patients in pathway C experienced significantly more grade 3/4 AEs during induction 1 (medians 16.0 [IQR: 8.0–20.5]) and induction 2 (15.0 [9.0–17.5]) compared to patients in pathways A (9.0 [6.0–11.0], p = 0.045 [induction 1] and 6.0 [3.0–8.0], p = 0.030 [induction 2]) and D (6.5 [5.5–10.0], p = 0.026 [induction 1] and 5.5 [3.5–8.5], p = 0.026 [induction 2]). More events were also seen for pathway B (10.0 [8.0–13.0], p = 0.023) than pathway D. Only 21/106 (19.8%) patients completed all protocol treatment. Discontinuation was highest during inductions 1 and 2; 27/106 (25.5%) and 11/106 (10.4%) mainly due to refractory/relapsed disease (19/38; 50%). Relapsed/refractory ALL was also the main reason for discontinuation of therapy at other timepoints (33/47; 70.2%) across all arms. Only five of 106 (4.7%) overtly stopped therapy due to toxicity.
A comparison of patient characteristics across the pathways is shown in Table 1. Participants on pathway D were significantly older than those on pathway B (median 73 years [IQR: 70–78] vs. 67 [IQR: 62–70], p = 0.0001), and had greater comorbidity; 9/21 (45%) with a Charleston Index of 7 or more in pathway D compared to only 8/51 (16.7%) in pathway B. The greater frailty of the pathway D group was also evident when comparing baseline QoL measures and comorbidities, with significantly lower physical functioning compared to pathway B; medians 60.0 (IQR: 53.3–80) versus 86.7 (IQR: 66.7–100), p = 0.014 (Tables S6 and S7). No patient with a Charleston index score of 7 or above was allocated to pathway C (p = 0.013). Major, age-associated comorbidities were common across the entire study cohort and included cardiac disease 27/121 (22.3%), diabetes 17/121 (14.0%), hypertension 39/121 (32.2%), and other cancer 22/121 (18.1%), eight of which were previous breast cancer and seven previous hematological malignancy.
Significant differences were seen in duration of inpatient stay, analysed by percentage of total treatment period spent in hospital (p = 0.026). Patients receiving pathways B and C spent more treatment-time in hospital compared to pathways A and D, with the effect most pronounced during induction (p = 0.0001) where pathway B and C participants were inpatients for 62.1% (46.3–96.7) and 75.8% (68.8–83.0), respectively compared to pathway A and D participants at 22.8% (IQR: 9.8–55.6) and 31.1% (IQR: 14.5–51.5), respectively. QoL was compared by pathway—summarized in supplementary results. We saw no indication that the least intensive pathway D provided a better QoL, with scores for some scales numerically lower than those of pathways A–C (Figure S4A–D). Any decreases in QoL from baseline were generally seen at the end of induction phases, with improvements in the FACT scores seen by the end of consolidation 1 and maintenance 1 (Table S8). Physical function scores, as assessed by QLQ-C30, remained reduced throughout while sensory and motor neuropathy scores increased at later points during therapy.
We compared the EFS and OS of UKALL60+ cohort with that of the 65 patients aged 60–65 years, treated on the full intensity adult ALL trial UKALL14 in an overlapping recruitment timeframe. Unsurprisingly, patients in UKALL14 had lower ECOG scores (40.0% vs. 60.9% ECOG 0, p = 0.0068). Fewer had baseline comorbidities (67.7% vs. 85.0%, p = 0.0059)—particularly notable for cardiac morbidities (6.2% vs. 22.5% p = 0.0046). Although CR rates were higher; UKALL14 55/63 (87.3%) vs. UKALL60+ 82/118 (69.2%), as shown in Table 1, EFS and OS rates at 3 years were 20.5% (11.5–31.3) and 25.2% (15.2–36.5) for UKALL14 and 18.8% (12.2–26.5) and 23.2% (15.9–31.4) for UKALL60+ (Figure 1C,D). However, the type of events differed, with only 18/55 (32.7%) being relapse, 9/55 deaths without remission, and 26/55 (47.2%) deaths in remission in UKALL14 compared to 56/95 (58.9%), 32/95 (33.7%), and 7/95 (7.4%) respectively, for UKALL60+. Among the UKALL14 60–65 year-old cohort, 28/65 had received allo-SCT, resulting in death in remission in 3/28 (46%).5 Among patients treated on pathway B, there was no difference in outcome between patients with high/very high-risk versus standard-risk genetics (EFS HR: 1.35 [0.68–2.67], p = 0.39) whereas there was a difference in outcome by genetic risk for patients aged 60–65 years old treated on UKALL14 (HR: 2.59 [1.12–5.98], p = 0.026).
Our survival data are broadly commensurate with data from a GMALL cohort of similar median age6 where OS at 3 years was 32%. However, the UKALL60+ population were in worse health overall; 27.5% had a Charlson Index >7 compared to the GMALL cohort, with only 11% scoring >3, commensurate with the GMALL exclusion criteria for comorbidities. By contrast to the GMALL early death rate of 14%, we observed a low treatment-related mortality. UKALL60+ treatments were successfully planned to minimize harm, but this did not improve OS.
It was unexpected that the 3-year EFS and OS of 20.5% and 25.2% for those aged 60–65 years treated on UKALL14 data did not differ from that of the UKALL60+ recruits, with completely overlapping survival curves (Figure 1). The outcomes are similar to those reported in an EBMT study of 418 patients aged over 55 years receiving alloSCT; 5-year LFS of 34% but a 51% nonrelapse mortality.7 Taken together, these data suggest even the most intensive treatments including alloSCT do not generate excellent outcomes for most older patients with ALL. We were surprised to see no evidence of better QoL for the recipients of the least intensive pathway D, despite a significant reduction in length of hospital stay.
In summary, the UKALL60+ pathways proved safe for initial cytoreduction, but the survival outcomes in this representative population of older patients with ALL was unsatisfactory. Nonchemotherapy approaches should be employed at the earliest opportunity for this patient group. QoL should always be measured, as the investigators assumptions do not necessarily reflect patients' experience.
Bela Patel: Trial design, trial management group member, manuscript writing. Amy A. Kirkwood: Trial design, lead statistician, data analysis, manuscript writing. Clare J. Rowntree: Trial management group member, site principal investigator. Krisztina Z. Alapi: Central lab manager, specimen processing, MRD analysis. Emilio Barretta: Central analysis of genetics. Laura Clifton-Hadley: Trial management group member, lead trial co-ordination. Tom Creasey: Central analysis of genetics. SooWah Lee: Specimen processing, MRD analysis. David I. Marks: Trial management group member, site principal investigator. Anthony V. Moorman: Trial management group member, central coordination of genetics. Nicholas Morley: Trial management group member, site principal investigator. Pip Patrick: Trial management group member, senior trial coordination. Zaynab Rana: Trial management group member, trial coordination. Anita Rijneveld: Site principal investigator, lead for HOVON. John A. Snowden: Trial management group member, quality of life lead. Adele K. Fielding: Trial concept and design, trial management group chair, trial chief investigator, manuscript writing, trial funding.
The authors declare no conflict of interest.
Cancer Research UK CRUK/A13920 to AKF, CRUK/A21019 to AKF/AVM, and an unrestricted educational support grant from Jazz Pharma.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


