Lauren E. Parker, Lillian Kang, Carmelo A. Milano, Alejandro A. Lobo, Julie W. Doberne, Muath Bishawi, Christopher. W. Jensen, Chetan B. Patel, Adam D. DeVore, Stuart D. Russell, Jason N. Katz, Jacob N. Schroder
{"title":"微轴血流泵治疗心源性休克:对血液动力学、溶血和末端器官恢复的影响","authors":"Lauren E. Parker, Lillian Kang, Carmelo A. Milano, Alejandro A. Lobo, Julie W. Doberne, Muath Bishawi, Christopher. W. Jensen, Chetan B. Patel, Adam D. DeVore, Stuart D. Russell, Jason N. Katz, Jacob N. Schroder","doi":"10.1155/2024/3584383","DOIUrl":null,"url":null,"abstract":"<div>\n <p><i>Background</i>. The Impella 5.5 offers a less invasive transvalvular approach to left ventricular mechanical support. End-organ recovery and hemolysis have been well-studied with durable left ventricular assist devices but effects of Impella 5.5 on these parameters are less well described. <i>Methods</i>. All Impella 5.5 recipients between August 2020 and June 2023 were reviewed from a single institution. Hemodynamics and laboratory values were compared between preimplant and prior to device removal. Hemolysis was defined as postoperative lactate dehydrogenase >1000 IU/L with concurrent plasma-free hemoglobin >50 mg/dL. Paired Wilcoxon tests compared the median of differences between preimplant and pre-explant values. <i>Results</i>. We studied 127 consecutive implants of the Impella 5.5. Thirty-one patients had concomitant VA-ECMO, and one received Impella 5.5 after durable LVAD explant; these cases were excluded. Our final cohort included 95 patients, with an average age of 55.29 ± 14.5 years. Median implant duration was 11 days (IQR:6–16 days). To avoid confounding hemodynamic factors, we restricted hemodynamic analysis to the 37 patients who received isolated Impella 5.5, excluding those with prior IABP, Impella CP, acute MI, or prior cardiac surgery. These patients experienced improvements from baseline in pulmonary vascular resistance (−77.03 dynes/sec/cm<sup>−5</sup>, <i>p</i> < 0.01) and wedge pressure (−6.5 mmHg, <i>p</i> < 0.01). Furthermore, cardiac index improved from baseline (+1.3, <i>p</i> < 0.01). In the total cohort (<i>n</i> = 95), pre-explant creatinine (−0.2 mg/dL, <i>p</i> < 0.01) and ALT (−9.0 mg/dL, <i>p</i> < 0.01) decreased relative to values before the implant. Twenty-three (24%) met criteria for hemolysis; however, none underwent device removal for clinically significant hemolysis. Takeback was required in 25 patients, 22 of which were for axillary hematoma. <i>Conclusions</i>. Impella 5.5 support acutely improved markers of end-organ function and hemodynamics, including PVR.</p>\n </div>","PeriodicalId":15367,"journal":{"name":"Journal of Cardiac Surgery","volume":"2024 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/3584383","citationCount":"0","resultStr":"{\"title\":\"Microaxial Flow Pumps for Cardiogenic Shock: Effects on Hemodynamics, Hemolysis, and End-Organ Recovery\",\"authors\":\"Lauren E. Parker, Lillian Kang, Carmelo A. Milano, Alejandro A. Lobo, Julie W. Doberne, Muath Bishawi, Christopher. W. Jensen, Chetan B. Patel, Adam D. DeVore, Stuart D. Russell, Jason N. Katz, Jacob N. Schroder\",\"doi\":\"10.1155/2024/3584383\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n <p><i>Background</i>. The Impella 5.5 offers a less invasive transvalvular approach to left ventricular mechanical support. End-organ recovery and hemolysis have been well-studied with durable left ventricular assist devices but effects of Impella 5.5 on these parameters are less well described. <i>Methods</i>. All Impella 5.5 recipients between August 2020 and June 2023 were reviewed from a single institution. Hemodynamics and laboratory values were compared between preimplant and prior to device removal. Hemolysis was defined as postoperative lactate dehydrogenase >1000 IU/L with concurrent plasma-free hemoglobin >50 mg/dL. Paired Wilcoxon tests compared the median of differences between preimplant and pre-explant values. <i>Results</i>. We studied 127 consecutive implants of the Impella 5.5. Thirty-one patients had concomitant VA-ECMO, and one received Impella 5.5 after durable LVAD explant; these cases were excluded. Our final cohort included 95 patients, with an average age of 55.29 ± 14.5 years. Median implant duration was 11 days (IQR:6–16 days). To avoid confounding hemodynamic factors, we restricted hemodynamic analysis to the 37 patients who received isolated Impella 5.5, excluding those with prior IABP, Impella CP, acute MI, or prior cardiac surgery. These patients experienced improvements from baseline in pulmonary vascular resistance (−77.03 dynes/sec/cm<sup>−5</sup>, <i>p</i> < 0.01) and wedge pressure (−6.5 mmHg, <i>p</i> < 0.01). Furthermore, cardiac index improved from baseline (+1.3, <i>p</i> < 0.01). In the total cohort (<i>n</i> = 95), pre-explant creatinine (−0.2 mg/dL, <i>p</i> < 0.01) and ALT (−9.0 mg/dL, <i>p</i> < 0.01) decreased relative to values before the implant. Twenty-three (24%) met criteria for hemolysis; however, none underwent device removal for clinically significant hemolysis. Takeback was required in 25 patients, 22 of which were for axillary hematoma. <i>Conclusions</i>. Impella 5.5 support acutely improved markers of end-organ function and hemodynamics, including PVR.</p>\\n </div>\",\"PeriodicalId\":15367,\"journal\":{\"name\":\"Journal of Cardiac Surgery\",\"volume\":\"2024 1\",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/3584383\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiac Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1155/2024/3584383\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiac Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/3584383","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Microaxial Flow Pumps for Cardiogenic Shock: Effects on Hemodynamics, Hemolysis, and End-Organ Recovery
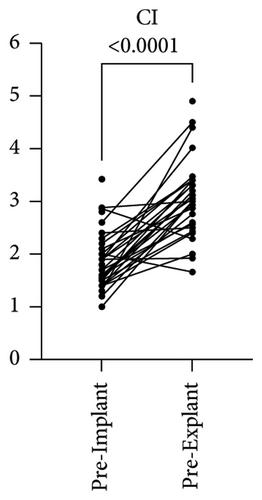
Background. The Impella 5.5 offers a less invasive transvalvular approach to left ventricular mechanical support. End-organ recovery and hemolysis have been well-studied with durable left ventricular assist devices but effects of Impella 5.5 on these parameters are less well described. Methods. All Impella 5.5 recipients between August 2020 and June 2023 were reviewed from a single institution. Hemodynamics and laboratory values were compared between preimplant and prior to device removal. Hemolysis was defined as postoperative lactate dehydrogenase >1000 IU/L with concurrent plasma-free hemoglobin >50 mg/dL. Paired Wilcoxon tests compared the median of differences between preimplant and pre-explant values. Results. We studied 127 consecutive implants of the Impella 5.5. Thirty-one patients had concomitant VA-ECMO, and one received Impella 5.5 after durable LVAD explant; these cases were excluded. Our final cohort included 95 patients, with an average age of 55.29 ± 14.5 years. Median implant duration was 11 days (IQR:6–16 days). To avoid confounding hemodynamic factors, we restricted hemodynamic analysis to the 37 patients who received isolated Impella 5.5, excluding those with prior IABP, Impella CP, acute MI, or prior cardiac surgery. These patients experienced improvements from baseline in pulmonary vascular resistance (−77.03 dynes/sec/cm−5, p < 0.01) and wedge pressure (−6.5 mmHg, p < 0.01). Furthermore, cardiac index improved from baseline (+1.3, p < 0.01). In the total cohort (n = 95), pre-explant creatinine (−0.2 mg/dL, p < 0.01) and ALT (−9.0 mg/dL, p < 0.01) decreased relative to values before the implant. Twenty-three (24%) met criteria for hemolysis; however, none underwent device removal for clinically significant hemolysis. Takeback was required in 25 patients, 22 of which were for axillary hematoma. Conclusions. Impella 5.5 support acutely improved markers of end-organ function and hemodynamics, including PVR.
期刊介绍:
Journal of Cardiac Surgery (JCS) is a peer-reviewed journal devoted to contemporary surgical treatment of cardiac disease. Renown for its detailed "how to" methods, JCS''s well-illustrated, concise technical articles, critical reviews and commentaries are highly valued by dedicated readers worldwide.
With Editor-in-Chief Harold Lazar, MD and an internationally prominent editorial board, JCS continues its 20-year history as an important professional resource. Editorial coverage includes biologic support, mechanical cardiac assist and/or replacement and surgical techniques, and features current material on topics such as OPCAB surgery, stented and stentless valves, endovascular stent placement, atrial fibrillation, transplantation, percutaneous valve repair/replacement, left ventricular restoration surgery, immunobiology, and bridges to transplant and recovery.
In addition, special sections (Images in Cardiac Surgery, Cardiac Regeneration) and historical reviews stimulate reader interest. The journal also routinely publishes proceedings of important international symposia in a timely manner.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


