Ai Demura, Kozue Takada, Hiroya Ohara, Toshi Sai, Masayuki Nakakura, Marisse Dy Dizon, Takeshi Satow, Masako Kinoshita
{"title":"局灶性皮质发育不良导致的额叶癫痫发作中无脑电图发作模式的头皮记录直流电位移。","authors":"Ai Demura, Kozue Takada, Hiroya Ohara, Toshi Sai, Masayuki Nakakura, Marisse Dy Dizon, Takeshi Satow, Masako Kinoshita","doi":"10.1002/epd2.20251","DOIUrl":null,"url":null,"abstract":"<p>Focal cortical dysplasia (FCD) is a major cause of intractable epilepsy, named on the basis of irregular dysmorphic neurons and ballooned cells within disorganized architecture of the neocortex.<span><sup>1</sup></span> Prominent astrocytosis is the common feature of FCD among various histopathological abnormalities of neuronal development.<span><sup>2</sup></span> In frontal lobe epilepsy, it is often difficult to localize seizure onset zones using scalp EEG.<span><sup>3</sup></span> Ictal direct current (DC) shifts reflect activities of neurons and glial cells, and helpful to delineate the epileptogenic zone.<span><sup>4-6</sup></span> We analyzed EEG data of a female patient with FCD in the right frontal lobe. While DC shifts during hyperkinetic seizures were useful in diagnosis, obvious EEG seizure patterns were not detected. Thus, DC shifts may raise diagnostic sensitivity.</p><p>A 33-year-old female, who developed generalized convulsion at the age of 17 years and presented with recent deterioration of seizures despite combination therapy of valproate, levetiracetam, and zonisamide, was investigated. Written informed consent was obtained from the patient for the participation and publication of the study. Brain MRI showed FCD in the right frontal lobe, anterior to the precentral gyrus, without contrast medium enhancement (Ingenia 3.0T CX; Philips Japan, Tokyo, Japan). Arterial spin labeling images show hyperperfusion of the lesion with post-labeling delay of both 1525 and 1800 ms (Figure 1A–C). Interictal Iodine-123-iomazenil single photon emission computed tomography showed decreased tracer uptake in the right frontal lobe.</p><p>Scalp record of video-EEG for 17 h was analyzed. EEG signals were recoded via silver/silver chloride disk electrodes (NE-116A; Nihon Kohden, Tokyo, Japan), 10 mm in diameter, placed on the scalp with adhesive paste (Ten20; Weaver and Company, Colorado, US) according to the International 10–20 system. The impedance of electrodes was kept less than 10 kΩ. Electrooculogram was recorded via an electrode placed 1 cm under right external canthus. Recording machines were EEG-1214 and EEG-1218 (Nihon Kohden, Tokyo, Japan). Sampling frequency was 500 Hz and 200 Hz, and bandpass filter for data acquisition was .08–120 Hz and .08–60 Hz, respectively.</p><p>Data were reviewed offline under conventional condition of time constant (TC) .3 s and clinical seizures with typical motor symptom were marked. Duration of each seizure was measured by visual inspection of video record and movement artifacts (Figure 1D, Figures S1 and S2). DC shifts were defined as negative slow deflection, better delineated with TC 2.0 s, 30 s/screen, and HF15 than conventional reviewing condition, and reproducible in location.<span><sup>7</sup></span> The amplitude was measured from DC shift onset to seizure onset of dystonic movement of the left arm (Figure 1E). The awake/sleep stages were classified according to the American Academy of Sleep Medicine manual version 2.5.<span><sup>8</sup></span></p><p>Twelve eligible seizures were analyzed. Her seizure semiology was comprised of abnormal sensation in the proximal part of the left arm, dystonic posture of the left side, hyperkinetic movement of the right side, and clonic convulsion of the left arm with preserved consciousness (Video 1). Ictal EEG reviewed in a conventional condition showed only ambiguous diffuse attenuation and low-voltage fast activities in frontocentral areas. By changing the reviewing condition (Figures S1 and S2), DC shifts were present on four occasions (33.3%) in the right fontal area. The amplitude of DC shifts was maximum at Fp2 (Table S1, Figure S3). Seizures with DC shifts showed significantly longer duration than those without (<i>p</i> = .046, unpaired <i>t</i>-test) (Figure 1F). Three out of four seizures with DC shifts occurred in sleep stage N2, whereas none of the seizures without DC shifts occurred in N2 (<i>p</i> = .018, Fisher's exact test) (Table S2). Add-on therapy with lacosamide completely suppressed her seizures. Hyperperfusion in arterial spin labeling images disappeared.</p><p>In this patient, scalp-recorded DC shifts during focal aware hyperkinetic seizures were useful in the diagnosis of frontal lobe, whereas ictal EEG reviewed in conventional condition showed only ambiguous diffuse electrodecremental patterns. In experimental seizure foci of cats, DC shifts distributed within 5 mm from the seizure focus and the amplitude was maximum at the focus.<span><sup>4</sup></span> Slow oscillation and negative deflection can reflect the glial membrane potential preceding to the paroxysmal depolarizing shifts in neocortical neurons.<span><sup>5</sup></span> In patients with medically intractable focal epilepsy, ictal DC shifts are helpful in delineating the epileptogenic zones.<span><sup>6, 7</sup></span> However, ictal DC shifts of this patient widely distribute maximum in Fp2 while FCD lesion resides in the right central area. The current findings resemble to pre-movement infraslow activities in faciobrachial dystonic seizures in leucine-rich glioma-inactivated one antibody-mediated encephalitis.<span><sup>9</sup></span> Previous reports in absence seizures showed that DC shift during typical 3 Hz generalized spike and wave complexes distributed with a negative–positive sequence in the frontal areas and opposite polarity in the posterior areas.<span><sup>10, 11</sup></span> In addition, diffuse electrodecremental pattern associated with poor surgical outcome.<span><sup>12</sup></span> Thus, ictal EEG characteristics of DC shift in our patient suggest an involvement of a widespread epileptic network instead of localized activity of the focal epileptogenic zone. Frequent emergence of DC shifts in N2 may indicate that seizure activities are enhanced in association with sleep network. The underlying mechanisms can relate to that of enlargement and change in the distribution of evoked potentials during sleep.<span><sup>13</sup></span></p><p>In conclusion, scalp-recorded ictal DC shifts during hyperkinetic seizures are useful in the diagnosis of focal aware seizures, especially in patients negative for EEG seizure patterns.</p><p>This study was partially supported by JSPS JPJSBP 120217720 and technology exchange grant by the Nakatani Foundation for Advancement of Measuring Technologies in Biomedical Engineering.</p>","PeriodicalId":50508,"journal":{"name":"Epileptic Disorders","volume":"26 5","pages":"711-714"},"PeriodicalIF":1.9000,"publicationDate":"2024-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/epd2.20251","citationCount":"0","resultStr":"{\"title\":\"Scalp-recorded direct current shifts without EEG seizure patterns in frontal lobe seizures due to focal cortical dysplasia\",\"authors\":\"Ai Demura, Kozue Takada, Hiroya Ohara, Toshi Sai, Masayuki Nakakura, Marisse Dy Dizon, Takeshi Satow, Masako Kinoshita\",\"doi\":\"10.1002/epd2.20251\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Focal cortical dysplasia (FCD) is a major cause of intractable epilepsy, named on the basis of irregular dysmorphic neurons and ballooned cells within disorganized architecture of the neocortex.<span><sup>1</sup></span> Prominent astrocytosis is the common feature of FCD among various histopathological abnormalities of neuronal development.<span><sup>2</sup></span> In frontal lobe epilepsy, it is often difficult to localize seizure onset zones using scalp EEG.<span><sup>3</sup></span> Ictal direct current (DC) shifts reflect activities of neurons and glial cells, and helpful to delineate the epileptogenic zone.<span><sup>4-6</sup></span> We analyzed EEG data of a female patient with FCD in the right frontal lobe. While DC shifts during hyperkinetic seizures were useful in diagnosis, obvious EEG seizure patterns were not detected. Thus, DC shifts may raise diagnostic sensitivity.</p><p>A 33-year-old female, who developed generalized convulsion at the age of 17 years and presented with recent deterioration of seizures despite combination therapy of valproate, levetiracetam, and zonisamide, was investigated. Written informed consent was obtained from the patient for the participation and publication of the study. Brain MRI showed FCD in the right frontal lobe, anterior to the precentral gyrus, without contrast medium enhancement (Ingenia 3.0T CX; Philips Japan, Tokyo, Japan). Arterial spin labeling images show hyperperfusion of the lesion with post-labeling delay of both 1525 and 1800 ms (Figure 1A–C). Interictal Iodine-123-iomazenil single photon emission computed tomography showed decreased tracer uptake in the right frontal lobe.</p><p>Scalp record of video-EEG for 17 h was analyzed. EEG signals were recoded via silver/silver chloride disk electrodes (NE-116A; Nihon Kohden, Tokyo, Japan), 10 mm in diameter, placed on the scalp with adhesive paste (Ten20; Weaver and Company, Colorado, US) according to the International 10–20 system. The impedance of electrodes was kept less than 10 kΩ. Electrooculogram was recorded via an electrode placed 1 cm under right external canthus. Recording machines were EEG-1214 and EEG-1218 (Nihon Kohden, Tokyo, Japan). Sampling frequency was 500 Hz and 200 Hz, and bandpass filter for data acquisition was .08–120 Hz and .08–60 Hz, respectively.</p><p>Data were reviewed offline under conventional condition of time constant (TC) .3 s and clinical seizures with typical motor symptom were marked. Duration of each seizure was measured by visual inspection of video record and movement artifacts (Figure 1D, Figures S1 and S2). DC shifts were defined as negative slow deflection, better delineated with TC 2.0 s, 30 s/screen, and HF15 than conventional reviewing condition, and reproducible in location.<span><sup>7</sup></span> The amplitude was measured from DC shift onset to seizure onset of dystonic movement of the left arm (Figure 1E). The awake/sleep stages were classified according to the American Academy of Sleep Medicine manual version 2.5.<span><sup>8</sup></span></p><p>Twelve eligible seizures were analyzed. Her seizure semiology was comprised of abnormal sensation in the proximal part of the left arm, dystonic posture of the left side, hyperkinetic movement of the right side, and clonic convulsion of the left arm with preserved consciousness (Video 1). Ictal EEG reviewed in a conventional condition showed only ambiguous diffuse attenuation and low-voltage fast activities in frontocentral areas. By changing the reviewing condition (Figures S1 and S2), DC shifts were present on four occasions (33.3%) in the right fontal area. The amplitude of DC shifts was maximum at Fp2 (Table S1, Figure S3). Seizures with DC shifts showed significantly longer duration than those without (<i>p</i> = .046, unpaired <i>t</i>-test) (Figure 1F). Three out of four seizures with DC shifts occurred in sleep stage N2, whereas none of the seizures without DC shifts occurred in N2 (<i>p</i> = .018, Fisher's exact test) (Table S2). Add-on therapy with lacosamide completely suppressed her seizures. Hyperperfusion in arterial spin labeling images disappeared.</p><p>In this patient, scalp-recorded DC shifts during focal aware hyperkinetic seizures were useful in the diagnosis of frontal lobe, whereas ictal EEG reviewed in conventional condition showed only ambiguous diffuse electrodecremental patterns. In experimental seizure foci of cats, DC shifts distributed within 5 mm from the seizure focus and the amplitude was maximum at the focus.<span><sup>4</sup></span> Slow oscillation and negative deflection can reflect the glial membrane potential preceding to the paroxysmal depolarizing shifts in neocortical neurons.<span><sup>5</sup></span> In patients with medically intractable focal epilepsy, ictal DC shifts are helpful in delineating the epileptogenic zones.<span><sup>6, 7</sup></span> However, ictal DC shifts of this patient widely distribute maximum in Fp2 while FCD lesion resides in the right central area. The current findings resemble to pre-movement infraslow activities in faciobrachial dystonic seizures in leucine-rich glioma-inactivated one antibody-mediated encephalitis.<span><sup>9</sup></span> Previous reports in absence seizures showed that DC shift during typical 3 Hz generalized spike and wave complexes distributed with a negative–positive sequence in the frontal areas and opposite polarity in the posterior areas.<span><sup>10, 11</sup></span> In addition, diffuse electrodecremental pattern associated with poor surgical outcome.<span><sup>12</sup></span> Thus, ictal EEG characteristics of DC shift in our patient suggest an involvement of a widespread epileptic network instead of localized activity of the focal epileptogenic zone. Frequent emergence of DC shifts in N2 may indicate that seizure activities are enhanced in association with sleep network. The underlying mechanisms can relate to that of enlargement and change in the distribution of evoked potentials during sleep.<span><sup>13</sup></span></p><p>In conclusion, scalp-recorded ictal DC shifts during hyperkinetic seizures are useful in the diagnosis of focal aware seizures, especially in patients negative for EEG seizure patterns.</p><p>This study was partially supported by JSPS JPJSBP 120217720 and technology exchange grant by the Nakatani Foundation for Advancement of Measuring Technologies in Biomedical Engineering.</p>\",\"PeriodicalId\":50508,\"journal\":{\"name\":\"Epileptic Disorders\",\"volume\":\"26 5\",\"pages\":\"711-714\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/epd2.20251\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Epileptic Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/epd2.20251\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epileptic Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/epd2.20251","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Scalp-recorded direct current shifts without EEG seizure patterns in frontal lobe seizures due to focal cortical dysplasia
Focal cortical dysplasia (FCD) is a major cause of intractable epilepsy, named on the basis of irregular dysmorphic neurons and ballooned cells within disorganized architecture of the neocortex.1 Prominent astrocytosis is the common feature of FCD among various histopathological abnormalities of neuronal development.2 In frontal lobe epilepsy, it is often difficult to localize seizure onset zones using scalp EEG.3 Ictal direct current (DC) shifts reflect activities of neurons and glial cells, and helpful to delineate the epileptogenic zone.4-6 We analyzed EEG data of a female patient with FCD in the right frontal lobe. While DC shifts during hyperkinetic seizures were useful in diagnosis, obvious EEG seizure patterns were not detected. Thus, DC shifts may raise diagnostic sensitivity.
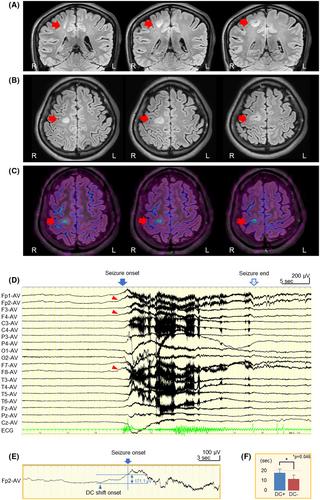
A 33-year-old female, who developed generalized convulsion at the age of 17 years and presented with recent deterioration of seizures despite combination therapy of valproate, levetiracetam, and zonisamide, was investigated. Written informed consent was obtained from the patient for the participation and publication of the study. Brain MRI showed FCD in the right frontal lobe, anterior to the precentral gyrus, without contrast medium enhancement (Ingenia 3.0T CX; Philips Japan, Tokyo, Japan). Arterial spin labeling images show hyperperfusion of the lesion with post-labeling delay of both 1525 and 1800 ms (Figure 1A–C). Interictal Iodine-123-iomazenil single photon emission computed tomography showed decreased tracer uptake in the right frontal lobe.
Scalp record of video-EEG for 17 h was analyzed. EEG signals were recoded via silver/silver chloride disk electrodes (NE-116A; Nihon Kohden, Tokyo, Japan), 10 mm in diameter, placed on the scalp with adhesive paste (Ten20; Weaver and Company, Colorado, US) according to the International 10–20 system. The impedance of electrodes was kept less than 10 kΩ. Electrooculogram was recorded via an electrode placed 1 cm under right external canthus. Recording machines were EEG-1214 and EEG-1218 (Nihon Kohden, Tokyo, Japan). Sampling frequency was 500 Hz and 200 Hz, and bandpass filter for data acquisition was .08–120 Hz and .08–60 Hz, respectively.
Data were reviewed offline under conventional condition of time constant (TC) .3 s and clinical seizures with typical motor symptom were marked. Duration of each seizure was measured by visual inspection of video record and movement artifacts (Figure 1D, Figures S1 and S2). DC shifts were defined as negative slow deflection, better delineated with TC 2.0 s, 30 s/screen, and HF15 than conventional reviewing condition, and reproducible in location.7 The amplitude was measured from DC shift onset to seizure onset of dystonic movement of the left arm (Figure 1E). The awake/sleep stages were classified according to the American Academy of Sleep Medicine manual version 2.5.8
Twelve eligible seizures were analyzed. Her seizure semiology was comprised of abnormal sensation in the proximal part of the left arm, dystonic posture of the left side, hyperkinetic movement of the right side, and clonic convulsion of the left arm with preserved consciousness (Video 1). Ictal EEG reviewed in a conventional condition showed only ambiguous diffuse attenuation and low-voltage fast activities in frontocentral areas. By changing the reviewing condition (Figures S1 and S2), DC shifts were present on four occasions (33.3%) in the right fontal area. The amplitude of DC shifts was maximum at Fp2 (Table S1, Figure S3). Seizures with DC shifts showed significantly longer duration than those without (p = .046, unpaired t-test) (Figure 1F). Three out of four seizures with DC shifts occurred in sleep stage N2, whereas none of the seizures without DC shifts occurred in N2 (p = .018, Fisher's exact test) (Table S2). Add-on therapy with lacosamide completely suppressed her seizures. Hyperperfusion in arterial spin labeling images disappeared.
In this patient, scalp-recorded DC shifts during focal aware hyperkinetic seizures were useful in the diagnosis of frontal lobe, whereas ictal EEG reviewed in conventional condition showed only ambiguous diffuse electrodecremental patterns. In experimental seizure foci of cats, DC shifts distributed within 5 mm from the seizure focus and the amplitude was maximum at the focus.4 Slow oscillation and negative deflection can reflect the glial membrane potential preceding to the paroxysmal depolarizing shifts in neocortical neurons.5 In patients with medically intractable focal epilepsy, ictal DC shifts are helpful in delineating the epileptogenic zones.6, 7 However, ictal DC shifts of this patient widely distribute maximum in Fp2 while FCD lesion resides in the right central area. The current findings resemble to pre-movement infraslow activities in faciobrachial dystonic seizures in leucine-rich glioma-inactivated one antibody-mediated encephalitis.9 Previous reports in absence seizures showed that DC shift during typical 3 Hz generalized spike and wave complexes distributed with a negative–positive sequence in the frontal areas and opposite polarity in the posterior areas.10, 11 In addition, diffuse electrodecremental pattern associated with poor surgical outcome.12 Thus, ictal EEG characteristics of DC shift in our patient suggest an involvement of a widespread epileptic network instead of localized activity of the focal epileptogenic zone. Frequent emergence of DC shifts in N2 may indicate that seizure activities are enhanced in association with sleep network. The underlying mechanisms can relate to that of enlargement and change in the distribution of evoked potentials during sleep.13
In conclusion, scalp-recorded ictal DC shifts during hyperkinetic seizures are useful in the diagnosis of focal aware seizures, especially in patients negative for EEG seizure patterns.
This study was partially supported by JSPS JPJSBP 120217720 and technology exchange grant by the Nakatani Foundation for Advancement of Measuring Technologies in Biomedical Engineering.
期刊介绍:
Epileptic Disorders is the leading forum where all experts and medical studentswho wish to improve their understanding of epilepsy and related disorders can share practical experiences surrounding diagnosis and care, natural history, and management of seizures.
Epileptic Disorders is the official E-journal of the International League Against Epilepsy for educational communication. As the journal celebrates its 20th anniversary, it will now be available only as an online version. Its mission is to create educational links between epileptologists and other health professionals in clinical practice and scientists or physicians in research-based institutions. This change is accompanied by an increase in the number of issues per year, from 4 to 6, to ensure regular diffusion of recently published material (high quality Review and Seminar in Epileptology papers; Original Research articles or Case reports of educational value; MultiMedia Teaching Material), to serve the global medical community that cares for those affected by epilepsy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


