Johanna M Ospel, Leon Rinkel, Aravind Ganesh, Andrew Demchuk, Manraj Heran, Eric Sauvageau, Manish Joshi, Diogo Haussen, Mahesh Jayaraman, Shelagh Coutts, Amy Yu, Volker Puetz, Dana Iancu, Oh Young Bang, Jason Tarpley, Staffan Holmin, Michael Kelly, Michael Tymianski, Michael Hill, Mayank Goyal
{"title":"急性缺血性卒中的定量组织成像结果与临床结果有何关系?","authors":"Johanna M Ospel, Leon Rinkel, Aravind Ganesh, Andrew Demchuk, Manraj Heran, Eric Sauvageau, Manish Joshi, Diogo Haussen, Mahesh Jayaraman, Shelagh Coutts, Amy Yu, Volker Puetz, Dana Iancu, Oh Young Bang, Jason Tarpley, Staffan Holmin, Michael Kelly, Michael Tymianski, Michael Hill, Mayank Goyal","doi":"10.5853/jos.2023.02180","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Infarct volume and other imaging markers are increasingly used as surrogate measures for clinical outcome in acute ischemic stroke research, but how improvements in these imaging surrogates translate into better clinical outcomes is currently unclear. We investigated how changes in infarct volume at 24 hours alter the probability of achieving good clinical outcome (modified Rankin Scale [mRS] 0-2).</p><p><strong>Methods: </strong>Data are from endovascular thrombectomy patients from the randomized controlled ESCAPE-NA1 (Efficacy and Safety of Nerinetide for the Treatment of Acute Ischaemic Stroke) trial. Infarct volume at 24 hours was manually segmented on non-contrast computed tomography or diffusion-weighted magnetic resonance imaging. Probabilities of achieving good outcome based on infarct volume were obtained from a multivariable logistic regression model. The probability of good outcome was plotted against infarct volume using linear spline regression.</p><p><strong>Results: </strong>A total of 1,099 patients were included in the analysis (median final infarct volume 24.9 mL [interquartile range: 6.6-92.2]). The relationship between total infarct volume and good outcome probability was nearly linear for infarct volumes between 0 mL and 250 mL. In this range, a 10% increase in the probability of achieving mRS 0-2 required a decrease in infarct volume of approximately 34.0 mL (95% confidence interval: -32.5 to -35.6). At infarct volumes above 250 mL, the probability of achieving mRS 0-2 probability was near zero. The relationships of tissue-specific infarct volumes and parenchymal hemorrhage volume generally showed similar patterns, although variability was high.</p><p><strong>Conclusion: </strong>There seems to be a near-linear association between total infarct volume and probability of achieving good outcome for infarcts up to 250 mL, whereas patients with infarct volumes greater than 250 mL are highly unlikely to have a favorable outcome.</p>","PeriodicalId":17135,"journal":{"name":"Journal of Stroke","volume":"26 2","pages":"252-259"},"PeriodicalIF":8.6000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11164591/pdf/","citationCount":"0","resultStr":"{\"title\":\"How Do Quantitative Tissue Imaging Outcomes in Acute Ischemic Stroke Relate to Clinical Outcomes?\",\"authors\":\"Johanna M Ospel, Leon Rinkel, Aravind Ganesh, Andrew Demchuk, Manraj Heran, Eric Sauvageau, Manish Joshi, Diogo Haussen, Mahesh Jayaraman, Shelagh Coutts, Amy Yu, Volker Puetz, Dana Iancu, Oh Young Bang, Jason Tarpley, Staffan Holmin, Michael Kelly, Michael Tymianski, Michael Hill, Mayank Goyal\",\"doi\":\"10.5853/jos.2023.02180\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>Infarct volume and other imaging markers are increasingly used as surrogate measures for clinical outcome in acute ischemic stroke research, but how improvements in these imaging surrogates translate into better clinical outcomes is currently unclear. We investigated how changes in infarct volume at 24 hours alter the probability of achieving good clinical outcome (modified Rankin Scale [mRS] 0-2).</p><p><strong>Methods: </strong>Data are from endovascular thrombectomy patients from the randomized controlled ESCAPE-NA1 (Efficacy and Safety of Nerinetide for the Treatment of Acute Ischaemic Stroke) trial. Infarct volume at 24 hours was manually segmented on non-contrast computed tomography or diffusion-weighted magnetic resonance imaging. Probabilities of achieving good outcome based on infarct volume were obtained from a multivariable logistic regression model. The probability of good outcome was plotted against infarct volume using linear spline regression.</p><p><strong>Results: </strong>A total of 1,099 patients were included in the analysis (median final infarct volume 24.9 mL [interquartile range: 6.6-92.2]). The relationship between total infarct volume and good outcome probability was nearly linear for infarct volumes between 0 mL and 250 mL. In this range, a 10% increase in the probability of achieving mRS 0-2 required a decrease in infarct volume of approximately 34.0 mL (95% confidence interval: -32.5 to -35.6). At infarct volumes above 250 mL, the probability of achieving mRS 0-2 probability was near zero. The relationships of tissue-specific infarct volumes and parenchymal hemorrhage volume generally showed similar patterns, although variability was high.</p><p><strong>Conclusion: </strong>There seems to be a near-linear association between total infarct volume and probability of achieving good outcome for infarcts up to 250 mL, whereas patients with infarct volumes greater than 250 mL are highly unlikely to have a favorable outcome.</p>\",\"PeriodicalId\":17135,\"journal\":{\"name\":\"Journal of Stroke\",\"volume\":\"26 2\",\"pages\":\"252-259\"},\"PeriodicalIF\":8.6000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11164591/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Stroke\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5853/jos.2023.02180\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5853/jos.2023.02180","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
How Do Quantitative Tissue Imaging Outcomes in Acute Ischemic Stroke Relate to Clinical Outcomes?
Background and purpose: Infarct volume and other imaging markers are increasingly used as surrogate measures for clinical outcome in acute ischemic stroke research, but how improvements in these imaging surrogates translate into better clinical outcomes is currently unclear. We investigated how changes in infarct volume at 24 hours alter the probability of achieving good clinical outcome (modified Rankin Scale [mRS] 0-2).
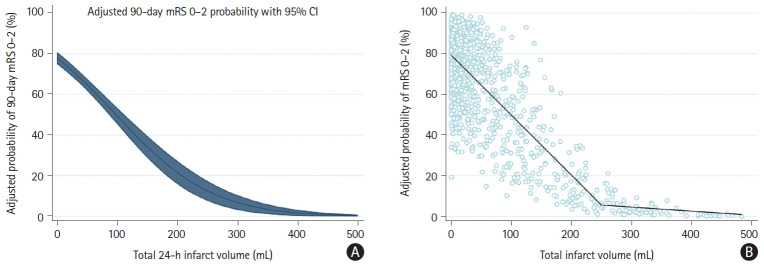
Methods: Data are from endovascular thrombectomy patients from the randomized controlled ESCAPE-NA1 (Efficacy and Safety of Nerinetide for the Treatment of Acute Ischaemic Stroke) trial. Infarct volume at 24 hours was manually segmented on non-contrast computed tomography or diffusion-weighted magnetic resonance imaging. Probabilities of achieving good outcome based on infarct volume were obtained from a multivariable logistic regression model. The probability of good outcome was plotted against infarct volume using linear spline regression.
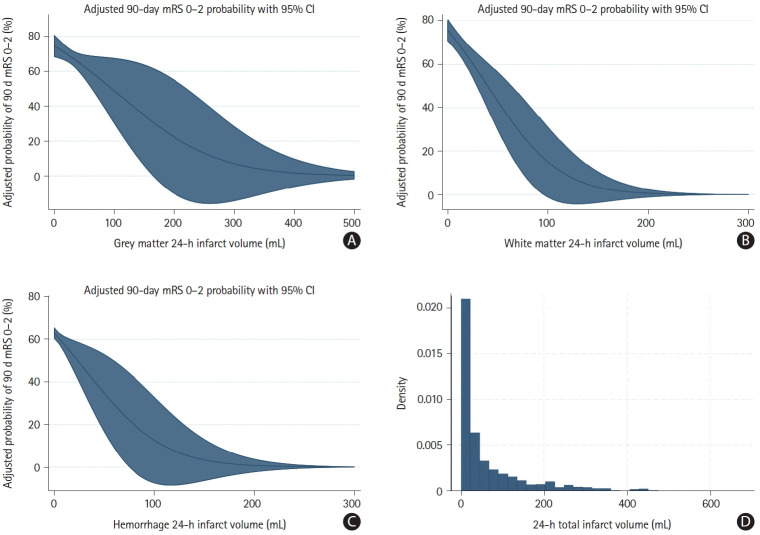
Results: A total of 1,099 patients were included in the analysis (median final infarct volume 24.9 mL [interquartile range: 6.6-92.2]). The relationship between total infarct volume and good outcome probability was nearly linear for infarct volumes between 0 mL and 250 mL. In this range, a 10% increase in the probability of achieving mRS 0-2 required a decrease in infarct volume of approximately 34.0 mL (95% confidence interval: -32.5 to -35.6). At infarct volumes above 250 mL, the probability of achieving mRS 0-2 probability was near zero. The relationships of tissue-specific infarct volumes and parenchymal hemorrhage volume generally showed similar patterns, although variability was high.
Conclusion: There seems to be a near-linear association between total infarct volume and probability of achieving good outcome for infarcts up to 250 mL, whereas patients with infarct volumes greater than 250 mL are highly unlikely to have a favorable outcome.
Journal of StrokeCLINICAL NEUROLOGYPERIPHERAL VASCULAR DISE-PERIPHERAL VASCULAR DISEASE
CiteScore
11.00
自引率
3.70%
发文量
52
审稿时长
12 weeks
期刊介绍:
The Journal of Stroke (JoS) is a peer-reviewed publication that focuses on clinical and basic investigation of cerebral circulation and associated diseases in stroke-related fields. Its aim is to enhance patient management, education, clinical or experimental research, and professionalism. The journal covers various areas of stroke research, including pathophysiology, risk factors, symptomatology, imaging, treatment, and rehabilitation. Basic science research is included when it provides clinically relevant information. The JoS is particularly interested in studies that highlight characteristics of stroke in the Asian population, as they are underrepresented in the literature.
The JoS had an impact factor of 8.2 in 2022 and aims to provide high-quality research papers to readers while maintaining a strong reputation. It is published three times a year, on the last day of January, May, and September. The online version of the journal is considered the main version as it includes all available content. Supplementary issues are occasionally published.
The journal is indexed in various databases, including SCI(E), Pubmed, PubMed Central, Scopus, KoreaMed, Komci, Synapse, Science Central, Google Scholar, and DOI/Crossref. It is also the official journal of the Korean Stroke Society since 1999, with the abbreviated title J Stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


