{"title":"平衡抗肥胖药物的创新性和可负担性:替代性体重维持计划的作用。","authors":"David D Kim, Jennifer H Hwang, A Mark Fendrick","doi":"10.1093/haschl/qxae055","DOIUrl":null,"url":null,"abstract":"<p><p>Despite remarkable clinical advances in highly effective anti-obesity medications, their high price and potential budget impact pose a major challenge in balancing equitable access and affordability. While most attention has been focused on the amount of weight loss achieved, less consideration has been paid to interventions to sustain weight loss after an individual stops losing weight. Using a policy simulation model, we quantified the impact of a weight-maintenance program following the weight-loss plateau from the initial full-dose glucagon-like peptide 1 (GLP-1) receptor agonists or incretin mimetic use. We measured long-term health care savings and the loss of some health benefits (eg, maintenance of weight loss, improvements in cardiometabolic risk factors, and reductions in diabetes and cardiovascular events). Our model suggested that, compared with continuous long-term full-dose GLP-1 receptor agonists or incretin mimetic drugs, the alternative weight-maintenance program would generate slightly fewer clinical benefits while generating substantial savings in lifetime health care spending. Using less expensive and potentially less effective alternative weight-maintenance programs may provide additional headroom to expand access to anti-obesity medications during the active weight-loss phase without increasing total health care spending.</p>","PeriodicalId":94025,"journal":{"name":"Health affairs scholar","volume":"2 6","pages":"qxae055"},"PeriodicalIF":2.7000,"publicationDate":"2024-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11138958/pdf/","citationCount":"0","resultStr":"{\"title\":\"Balancing innovation and affordability in anti-obesity medications: the role of an alternative weight-maintenance program.\",\"authors\":\"David D Kim, Jennifer H Hwang, A Mark Fendrick\",\"doi\":\"10.1093/haschl/qxae055\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Despite remarkable clinical advances in highly effective anti-obesity medications, their high price and potential budget impact pose a major challenge in balancing equitable access and affordability. While most attention has been focused on the amount of weight loss achieved, less consideration has been paid to interventions to sustain weight loss after an individual stops losing weight. Using a policy simulation model, we quantified the impact of a weight-maintenance program following the weight-loss plateau from the initial full-dose glucagon-like peptide 1 (GLP-1) receptor agonists or incretin mimetic use. We measured long-term health care savings and the loss of some health benefits (eg, maintenance of weight loss, improvements in cardiometabolic risk factors, and reductions in diabetes and cardiovascular events). Our model suggested that, compared with continuous long-term full-dose GLP-1 receptor agonists or incretin mimetic drugs, the alternative weight-maintenance program would generate slightly fewer clinical benefits while generating substantial savings in lifetime health care spending. Using less expensive and potentially less effective alternative weight-maintenance programs may provide additional headroom to expand access to anti-obesity medications during the active weight-loss phase without increasing total health care spending.</p>\",\"PeriodicalId\":94025,\"journal\":{\"name\":\"Health affairs scholar\",\"volume\":\"2 6\",\"pages\":\"qxae055\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11138958/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health affairs scholar\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/haschl/qxae055\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health affairs scholar","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/haschl/qxae055","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Balancing innovation and affordability in anti-obesity medications: the role of an alternative weight-maintenance program.
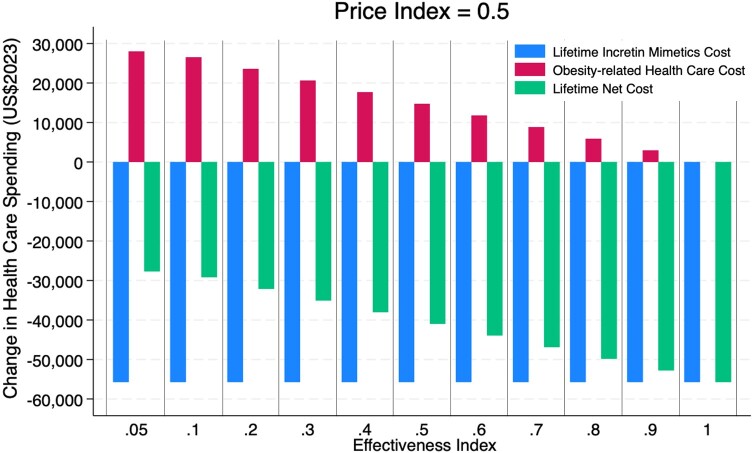
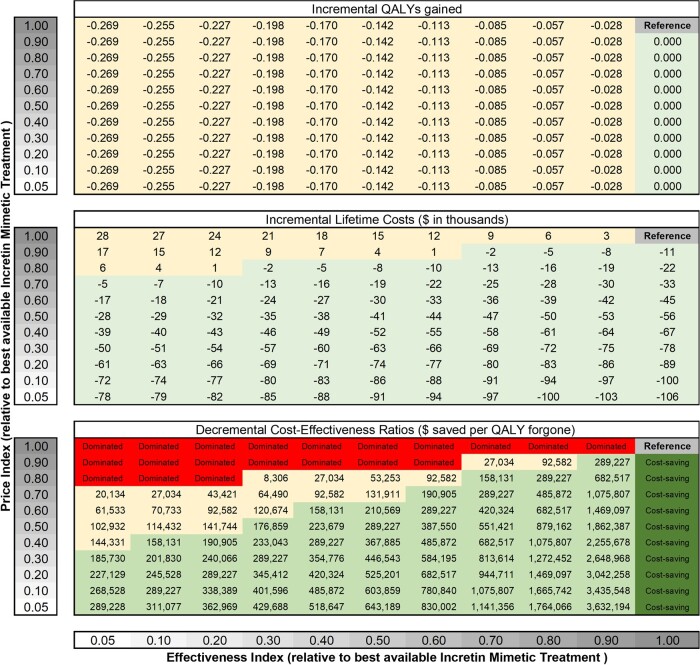
Despite remarkable clinical advances in highly effective anti-obesity medications, their high price and potential budget impact pose a major challenge in balancing equitable access and affordability. While most attention has been focused on the amount of weight loss achieved, less consideration has been paid to interventions to sustain weight loss after an individual stops losing weight. Using a policy simulation model, we quantified the impact of a weight-maintenance program following the weight-loss plateau from the initial full-dose glucagon-like peptide 1 (GLP-1) receptor agonists or incretin mimetic use. We measured long-term health care savings and the loss of some health benefits (eg, maintenance of weight loss, improvements in cardiometabolic risk factors, and reductions in diabetes and cardiovascular events). Our model suggested that, compared with continuous long-term full-dose GLP-1 receptor agonists or incretin mimetic drugs, the alternative weight-maintenance program would generate slightly fewer clinical benefits while generating substantial savings in lifetime health care spending. Using less expensive and potentially less effective alternative weight-maintenance programs may provide additional headroom to expand access to anti-obesity medications during the active weight-loss phase without increasing total health care spending.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


