Angela R. Wateska MPH, Mary Patricia Nowalk PhD, RDN, Shoroq M. Altawalbeh PharmD, PhD, Chyongchiou J. Lin PhD, MS, Lee H. Harrison MD, William Schaffner MD, Richard K. Zimmerman MD, MPH, Kenneth J. Smith MD, MS
{"title":"肺炎球菌疫苗接种成本效益的变化以及提高美国老年人接种率的计划。","authors":"Angela R. Wateska MPH, Mary Patricia Nowalk PhD, RDN, Shoroq M. Altawalbeh PharmD, PhD, Chyongchiou J. Lin PhD, MS, Lee H. Harrison MD, William Schaffner MD, Richard K. Zimmerman MD, MPH, Kenneth J. Smith MD, MS","doi":"10.1111/jgs.19031","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Multiple factors, such as less complex U.S. adult pneumococcal recommendations that could increase vaccination rates, childhood pneumococcal vaccination indirect effects that decrease adult vaccination impact, and increased vaccine hesitancy (particularly in underserved minorities), could diminish the cost-effectiveness of programs to increase pneumococcal vaccination in older adults. Prior analyses supported the economic favorability of these programs.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A Markov model compared no vaccination and current recommendations (either 20-valent pneumococcal conjugate vaccine [PCV20] alone or 15-valent pneumococcal conjugate vaccine plus the 23-valent pneumococcal polysaccharide vaccine [PCV15/PPSV23]) without or with programs to increase vaccine uptake in Black and non-Black 65-year-old cohorts. Pre-pandemic population- and serotype-specific pneumococcal disease risk and illness/vaccine costs came from U.S. databases. Program costs were $2.19 per vaccine-eligible person and increased absolute vaccination likelihood by 7.5%. Delphi panel estimates and trial data informed vaccine effectiveness values. Analyses took a healthcare perspective, discounting at 3%/year over a lifetime time horizon.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Uptake programs decreased pneumococcal disease overall. In Black cohorts, PCV20 without program cost $216,805 per quality-adjusted life year (QALY) gained compared with no vaccination; incremental cost-effectiveness was $245,546/QALY for PCV20 with program and $425,264/QALY for PCV15/PPSV23 with program. In non-Black cohorts, all strategies cost >$200,000/QALY gained. When considering the potential indirect effects from childhood vaccination, all strategies became less economically attractive. Increased vaccination with less complex strategies had negligible effects. In probabilistic sensitivity analyses, current recommendations with or without programs were unlikely to be favored at thresholds <$200,000/QALY gained.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Current U.S. pneumococcal vaccination recommendations for older adults were unlikely to be economically reasonable with or without programs to increase vaccine uptake. Alternatives to current pneumococcal vaccines that include pneumococcal serotypes associated with adult disease should be considered.</p>\n </section>\n </div>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 8","pages":"2423-2433"},"PeriodicalIF":4.3000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19031","citationCount":"0","resultStr":"{\"title\":\"Changes in the cost-effectiveness of pneumococcal vaccination and of programs to increase its uptake in U.S. older adults\",\"authors\":\"Angela R. Wateska MPH, Mary Patricia Nowalk PhD, RDN, Shoroq M. Altawalbeh PharmD, PhD, Chyongchiou J. Lin PhD, MS, Lee H. Harrison MD, William Schaffner MD, Richard K. Zimmerman MD, MPH, Kenneth J. Smith MD, MS\",\"doi\":\"10.1111/jgs.19031\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Multiple factors, such as less complex U.S. adult pneumococcal recommendations that could increase vaccination rates, childhood pneumococcal vaccination indirect effects that decrease adult vaccination impact, and increased vaccine hesitancy (particularly in underserved minorities), could diminish the cost-effectiveness of programs to increase pneumococcal vaccination in older adults. Prior analyses supported the economic favorability of these programs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A Markov model compared no vaccination and current recommendations (either 20-valent pneumococcal conjugate vaccine [PCV20] alone or 15-valent pneumococcal conjugate vaccine plus the 23-valent pneumococcal polysaccharide vaccine [PCV15/PPSV23]) without or with programs to increase vaccine uptake in Black and non-Black 65-year-old cohorts. Pre-pandemic population- and serotype-specific pneumococcal disease risk and illness/vaccine costs came from U.S. databases. Program costs were $2.19 per vaccine-eligible person and increased absolute vaccination likelihood by 7.5%. Delphi panel estimates and trial data informed vaccine effectiveness values. Analyses took a healthcare perspective, discounting at 3%/year over a lifetime time horizon.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Uptake programs decreased pneumococcal disease overall. In Black cohorts, PCV20 without program cost $216,805 per quality-adjusted life year (QALY) gained compared with no vaccination; incremental cost-effectiveness was $245,546/QALY for PCV20 with program and $425,264/QALY for PCV15/PPSV23 with program. In non-Black cohorts, all strategies cost >$200,000/QALY gained. When considering the potential indirect effects from childhood vaccination, all strategies became less economically attractive. Increased vaccination with less complex strategies had negligible effects. In probabilistic sensitivity analyses, current recommendations with or without programs were unlikely to be favored at thresholds <$200,000/QALY gained.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Current U.S. pneumococcal vaccination recommendations for older adults were unlikely to be economically reasonable with or without programs to increase vaccine uptake. Alternatives to current pneumococcal vaccines that include pneumococcal serotypes associated with adult disease should be considered.</p>\\n </section>\\n </div>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"72 8\",\"pages\":\"2423-2433\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19031\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19031\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19031","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Changes in the cost-effectiveness of pneumococcal vaccination and of programs to increase its uptake in U.S. older adults
Background
Multiple factors, such as less complex U.S. adult pneumococcal recommendations that could increase vaccination rates, childhood pneumococcal vaccination indirect effects that decrease adult vaccination impact, and increased vaccine hesitancy (particularly in underserved minorities), could diminish the cost-effectiveness of programs to increase pneumococcal vaccination in older adults. Prior analyses supported the economic favorability of these programs.
Methods
A Markov model compared no vaccination and current recommendations (either 20-valent pneumococcal conjugate vaccine [PCV20] alone or 15-valent pneumococcal conjugate vaccine plus the 23-valent pneumococcal polysaccharide vaccine [PCV15/PPSV23]) without or with programs to increase vaccine uptake in Black and non-Black 65-year-old cohorts. Pre-pandemic population- and serotype-specific pneumococcal disease risk and illness/vaccine costs came from U.S. databases. Program costs were $2.19 per vaccine-eligible person and increased absolute vaccination likelihood by 7.5%. Delphi panel estimates and trial data informed vaccine effectiveness values. Analyses took a healthcare perspective, discounting at 3%/year over a lifetime time horizon.
Results
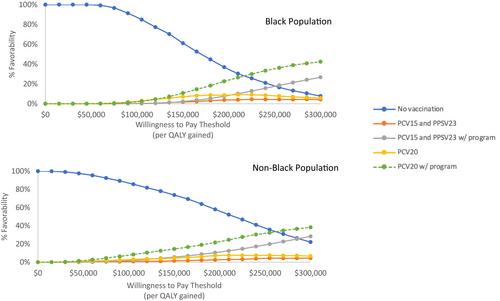
Uptake programs decreased pneumococcal disease overall. In Black cohorts, PCV20 without program cost $216,805 per quality-adjusted life year (QALY) gained compared with no vaccination; incremental cost-effectiveness was $245,546/QALY for PCV20 with program and $425,264/QALY for PCV15/PPSV23 with program. In non-Black cohorts, all strategies cost >$200,000/QALY gained. When considering the potential indirect effects from childhood vaccination, all strategies became less economically attractive. Increased vaccination with less complex strategies had negligible effects. In probabilistic sensitivity analyses, current recommendations with or without programs were unlikely to be favored at thresholds <$200,000/QALY gained.
Conclusion
Current U.S. pneumococcal vaccination recommendations for older adults were unlikely to be economically reasonable with or without programs to increase vaccine uptake. Alternatives to current pneumococcal vaccines that include pneumococcal serotypes associated with adult disease should be considered.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


