Julia H. Yuan MD, Dena E. Rifkin MD, MS, Charles Ginsberg MD, MAS, Peggy M. Cawthon PhD, MPH, Deborah M. Kado MD, MS, Scott R. Bauer MD, ScM, Kristine E. Ensrud MD, MPH, Andrew R. Hoffman MD, O. Alison Potok MD
{"title":"肾功能胱抑素 C 与肌酐之间的差异以及与肌肉质量和虚弱的关系。","authors":"Julia H. Yuan MD, Dena E. Rifkin MD, MS, Charles Ginsberg MD, MAS, Peggy M. Cawthon PhD, MPH, Deborah M. Kado MD, MS, Scott R. Bauer MD, ScM, Kristine E. Ensrud MD, MPH, Andrew R. Hoffman MD, O. Alison Potok MD","doi":"10.1111/jgs.19014","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>A higher difference in estimated glomerular filtration rate by cystatin C versus creatinine (eGFRDiff = eGFRCys – eGFRCreat) is associated with decreased frailty risk. Since eGFRCreat is influenced by muscle more than eGFRCys, muscle mass may explain this association. Previous work could not account for this when considering regional muscle measures by imaging. Deuterated creatine (D<sub>3</sub>Cr) dilution measures whole body muscle mass (kilograms). We aimed to determine whether eGFRDiff is associated with D<sub>3</sub>Cr muscle mass and whether muscle mass explains the association between eGFRDiff and frailty.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Cross-sectional analysis within the multicenter MrOS Study at Year 14 (visit 4). 490 men of the original cohort of 5994 MrOS participants (aged ≥65 at enrollment) were included. Exposure was eGFRDiff (= eGFRCys – eGFRCreat), calculated using CKD-EPI equations 2012/2021. Primary outcome was D<sub>3</sub>Cr muscle mass. Secondary outcome was phenotypic pre-frailty (one or two criteria) and frailty (≥three criteria) including the following: weight loss, weakness, slow gait, physical activity, poor energy. The association of eGFRDiff with D<sub>3</sub>Cr muscle mass was examined by linear regression, that with prefrailty / frailty by multinomial logistic regression.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Mean ± SD age was 84 ± 4 years, eGFRCreat 68 ± 16, eGFRCys 52 ± 16, eGFRDiff −15 ± 12 mL/min/1.73 m<sup>2</sup> and D<sub>3</sub>Cr muscle mass 24 ± 4 kg. For each SD increment in eGFRDiff, D3Cr muscle mass was 1.4 kg higher on average, <i>p</i> < 0.0001 (fully adjusted). Higher eGFRDiff was associated with lower odds of frailty (OR = 0.63 95% CI [0.45;0.89]), but this was partially attenuated and insignificant after additionally adjusting for D<sub>3</sub>Cr muscle mass (OR = 0.85 95% CI [0.58; 1.24]).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Higher eGFRDiff is associated with lower odds of frailty among late-life men. D<sub>3</sub>Cr muscle mass accounts for some of this association. This suggests that non-GFR determinants of creatinine and cystatin C, such as muscle mass, play a role in explaining the association of eGFRDiff with frailty. Future studies are needed to confirm.</p>\n </section>\n </div>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 10","pages":"3163-3170"},"PeriodicalIF":4.3000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11461133/pdf/","citationCount":"0","resultStr":"{\"title\":\"Difference between kidney function by cystatin C versus creatinine and association with muscle mass and frailty\",\"authors\":\"Julia H. Yuan MD, Dena E. Rifkin MD, MS, Charles Ginsberg MD, MAS, Peggy M. Cawthon PhD, MPH, Deborah M. Kado MD, MS, Scott R. Bauer MD, ScM, Kristine E. Ensrud MD, MPH, Andrew R. Hoffman MD, O. Alison Potok MD\",\"doi\":\"10.1111/jgs.19014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>A higher difference in estimated glomerular filtration rate by cystatin C versus creatinine (eGFRDiff = eGFRCys – eGFRCreat) is associated with decreased frailty risk. Since eGFRCreat is influenced by muscle more than eGFRCys, muscle mass may explain this association. Previous work could not account for this when considering regional muscle measures by imaging. Deuterated creatine (D<sub>3</sub>Cr) dilution measures whole body muscle mass (kilograms). We aimed to determine whether eGFRDiff is associated with D<sub>3</sub>Cr muscle mass and whether muscle mass explains the association between eGFRDiff and frailty.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Cross-sectional analysis within the multicenter MrOS Study at Year 14 (visit 4). 490 men of the original cohort of 5994 MrOS participants (aged ≥65 at enrollment) were included. Exposure was eGFRDiff (= eGFRCys – eGFRCreat), calculated using CKD-EPI equations 2012/2021. Primary outcome was D<sub>3</sub>Cr muscle mass. Secondary outcome was phenotypic pre-frailty (one or two criteria) and frailty (≥three criteria) including the following: weight loss, weakness, slow gait, physical activity, poor energy. The association of eGFRDiff with D<sub>3</sub>Cr muscle mass was examined by linear regression, that with prefrailty / frailty by multinomial logistic regression.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Mean ± SD age was 84 ± 4 years, eGFRCreat 68 ± 16, eGFRCys 52 ± 16, eGFRDiff −15 ± 12 mL/min/1.73 m<sup>2</sup> and D<sub>3</sub>Cr muscle mass 24 ± 4 kg. For each SD increment in eGFRDiff, D3Cr muscle mass was 1.4 kg higher on average, <i>p</i> < 0.0001 (fully adjusted). Higher eGFRDiff was associated with lower odds of frailty (OR = 0.63 95% CI [0.45;0.89]), but this was partially attenuated and insignificant after additionally adjusting for D<sub>3</sub>Cr muscle mass (OR = 0.85 95% CI [0.58; 1.24]).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Higher eGFRDiff is associated with lower odds of frailty among late-life men. D<sub>3</sub>Cr muscle mass accounts for some of this association. This suggests that non-GFR determinants of creatinine and cystatin C, such as muscle mass, play a role in explaining the association of eGFRDiff with frailty. Future studies are needed to confirm.</p>\\n </section>\\n </div>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"72 10\",\"pages\":\"3163-3170\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-05-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11461133/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19014\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19014","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Difference between kidney function by cystatin C versus creatinine and association with muscle mass and frailty
Background
A higher difference in estimated glomerular filtration rate by cystatin C versus creatinine (eGFRDiff = eGFRCys – eGFRCreat) is associated with decreased frailty risk. Since eGFRCreat is influenced by muscle more than eGFRCys, muscle mass may explain this association. Previous work could not account for this when considering regional muscle measures by imaging. Deuterated creatine (D3Cr) dilution measures whole body muscle mass (kilograms). We aimed to determine whether eGFRDiff is associated with D3Cr muscle mass and whether muscle mass explains the association between eGFRDiff and frailty.
Methods
Cross-sectional analysis within the multicenter MrOS Study at Year 14 (visit 4). 490 men of the original cohort of 5994 MrOS participants (aged ≥65 at enrollment) were included. Exposure was eGFRDiff (= eGFRCys – eGFRCreat), calculated using CKD-EPI equations 2012/2021. Primary outcome was D3Cr muscle mass. Secondary outcome was phenotypic pre-frailty (one or two criteria) and frailty (≥three criteria) including the following: weight loss, weakness, slow gait, physical activity, poor energy. The association of eGFRDiff with D3Cr muscle mass was examined by linear regression, that with prefrailty / frailty by multinomial logistic regression.
Results
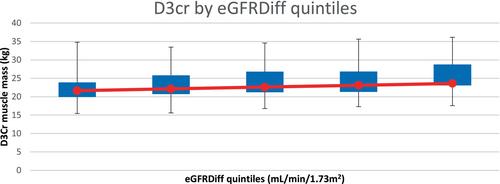
Mean ± SD age was 84 ± 4 years, eGFRCreat 68 ± 16, eGFRCys 52 ± 16, eGFRDiff −15 ± 12 mL/min/1.73 m2 and D3Cr muscle mass 24 ± 4 kg. For each SD increment in eGFRDiff, D3Cr muscle mass was 1.4 kg higher on average, p < 0.0001 (fully adjusted). Higher eGFRDiff was associated with lower odds of frailty (OR = 0.63 95% CI [0.45;0.89]), but this was partially attenuated and insignificant after additionally adjusting for D3Cr muscle mass (OR = 0.85 95% CI [0.58; 1.24]).
Conclusions
Higher eGFRDiff is associated with lower odds of frailty among late-life men. D3Cr muscle mass accounts for some of this association. This suggests that non-GFR determinants of creatinine and cystatin C, such as muscle mass, play a role in explaining the association of eGFRDiff with frailty. Future studies are needed to confirm.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


