Ajami Gikandi, Peter Chiu, Jordan Secor, Meena Nathan, Edward O'Leary, Edward Walsh, Tal Geva, Rebecca Beroukhim, Pedro Del Nido
{"title":"儿童大脑室纤维瘤手术切除术","authors":"Ajami Gikandi, Peter Chiu, Jordan Secor, Meena Nathan, Edward O'Leary, Edward Walsh, Tal Geva, Rebecca Beroukhim, Pedro Del Nido","doi":"10.1016/j.jtcvs.2024.05.013","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aims to provide an update on the clinical presentation, diagnostic workup, operative strategies, and midterm outcomes in children undergoing ventricular fibroma resection.</p><p><strong>Methods: </strong>Single-center, retrospective cohort study of patients undergoing ventricular fibroma resection between 2000 and 2023.</p><p><strong>Results: </strong>Among 52 patients, median age at surgery was 2.0 years (interquartile range, 0.8-4.6) and median tumor volume index was 69 mL/m<sup>2</sup> (interquartile range, 49-169). Tumor distorted the atrioventricular valve/subvalvar apparatus in 30 patients (58%) and abutted major epicardial coronary arteries in 41 patients (79%). Surgery was indicated for arrythmia (n = 45, 86%), symptoms (n = 14, 27%), or hemodynamic compromise (n = 11, 21%). Tumor was debulked in 34 patients (65%), including the last 21 patients. Concomitant atrioventricular valvuloplasty was performed in 18 patients and ventricular cavity closure in 15 patients (29%). During a median follow-up of 2.4 years (interquartile range, 0.8-6.2), there was no mortality, cardiac arrests, heart transplants, or single ventricle palliation. The 15-year risk of reoperation and clinical ventricular tachycardia/fibrillation was 6.7% (95% CI, 0-14.3) and 2.4% (95% CI, 0-7.2), respectively. On latest imaging, pre- and postdebulking left ventricular ejection fraction did not significantly differ (P = .069), whereas no patients had signs of outflow tract obstruction, inflow tract obstruction, or moderate or greater atrioventricular valve regurgitation.</p><p><strong>Conclusions: </strong>Large ventricular fibromas can be resected safely with appropriate surgical planning and an emphasis on debulking. Most children maintain left ventricular function and remain free of recurrent ventricular arrhythmias at follow-up. Extended follow-up is warranted to understand whether patients remain at risk for scar-based ventricular arrhythmias in the future.</p>","PeriodicalId":49975,"journal":{"name":"Journal of Thoracic and Cardiovascular Surgery","volume":" ","pages":"186-194"},"PeriodicalIF":4.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Surgical debulking of large ventricular fibromas in children.\",\"authors\":\"Ajami Gikandi, Peter Chiu, Jordan Secor, Meena Nathan, Edward O'Leary, Edward Walsh, Tal Geva, Rebecca Beroukhim, Pedro Del Nido\",\"doi\":\"10.1016/j.jtcvs.2024.05.013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study aims to provide an update on the clinical presentation, diagnostic workup, operative strategies, and midterm outcomes in children undergoing ventricular fibroma resection.</p><p><strong>Methods: </strong>Single-center, retrospective cohort study of patients undergoing ventricular fibroma resection between 2000 and 2023.</p><p><strong>Results: </strong>Among 52 patients, median age at surgery was 2.0 years (interquartile range, 0.8-4.6) and median tumor volume index was 69 mL/m<sup>2</sup> (interquartile range, 49-169). Tumor distorted the atrioventricular valve/subvalvar apparatus in 30 patients (58%) and abutted major epicardial coronary arteries in 41 patients (79%). Surgery was indicated for arrythmia (n = 45, 86%), symptoms (n = 14, 27%), or hemodynamic compromise (n = 11, 21%). Tumor was debulked in 34 patients (65%), including the last 21 patients. Concomitant atrioventricular valvuloplasty was performed in 18 patients and ventricular cavity closure in 15 patients (29%). During a median follow-up of 2.4 years (interquartile range, 0.8-6.2), there was no mortality, cardiac arrests, heart transplants, or single ventricle palliation. The 15-year risk of reoperation and clinical ventricular tachycardia/fibrillation was 6.7% (95% CI, 0-14.3) and 2.4% (95% CI, 0-7.2), respectively. On latest imaging, pre- and postdebulking left ventricular ejection fraction did not significantly differ (P = .069), whereas no patients had signs of outflow tract obstruction, inflow tract obstruction, or moderate or greater atrioventricular valve regurgitation.</p><p><strong>Conclusions: </strong>Large ventricular fibromas can be resected safely with appropriate surgical planning and an emphasis on debulking. Most children maintain left ventricular function and remain free of recurrent ventricular arrhythmias at follow-up. Extended follow-up is warranted to understand whether patients remain at risk for scar-based ventricular arrhythmias in the future.</p>\",\"PeriodicalId\":49975,\"journal\":{\"name\":\"Journal of Thoracic and Cardiovascular Surgery\",\"volume\":\" \",\"pages\":\"186-194\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1016/j.jtcvs.2024.05.013\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jtcvs.2024.05.013","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/25 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
研究目的本研究旨在更新接受室管膜纤维瘤切除术的儿童的临床表现、诊断工作、手术策略和中期预后:对2000年至2023年间接受室管膜纤维瘤切除术的患者进行单中心回顾性队列研究:52名患者中,手术年龄中位数为2.0岁(IQR 0.8-4.6),肿瘤体积指数中位数为69毫升/平方米(IQR 49-169)。30例(58%)患者的肿瘤扭曲了房室(AV)瓣/瓣下装置,41例(79%)患者的肿瘤与主要的心外膜冠状动脉相邻。手术指征为心律失常(45 例,占 86%)、症状(14 例,占 27%)和/或血流动力学受损(11 例,占 21%)。包括最后 21 名患者在内的 34 名患者(65%)进行了肿瘤剥除手术。18名患者同时进行了房室瓣成形术,15名(29%)患者进行了心室腔关闭术。在中位 2.4 年(IQR 0.8-6.2)的随访期间,没有发生死亡、心脏骤停、心脏移植或单心室姑息治疗。再次手术和临床室速/室颤的15年风险分别为6.7%(95% CI 0-14.3%)和2.4%(95% CI 0-7.2%)。在最新的影像学检查中,清除前和清除后的左心室射血分数没有显著差异(P=0.069),没有患者出现流出道梗阻、流入道梗阻或中度以上房室瓣反流:结论:只要制定适当的手术计划并注重剥离,大型心室纤维瘤是可以安全切除的。大多数患儿都能保持左心室功能,随访时也不会复发室性心律失常。为了解患者今后是否仍有发生瘢痕性室性心律失常的风险,有必要延长随访时间。
Surgical debulking of large ventricular fibromas in children.
Objective: This study aims to provide an update on the clinical presentation, diagnostic workup, operative strategies, and midterm outcomes in children undergoing ventricular fibroma resection.
Methods: Single-center, retrospective cohort study of patients undergoing ventricular fibroma resection between 2000 and 2023.
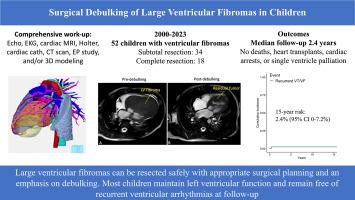
Results: Among 52 patients, median age at surgery was 2.0 years (interquartile range, 0.8-4.6) and median tumor volume index was 69 mL/m2 (interquartile range, 49-169). Tumor distorted the atrioventricular valve/subvalvar apparatus in 30 patients (58%) and abutted major epicardial coronary arteries in 41 patients (79%). Surgery was indicated for arrythmia (n = 45, 86%), symptoms (n = 14, 27%), or hemodynamic compromise (n = 11, 21%). Tumor was debulked in 34 patients (65%), including the last 21 patients. Concomitant atrioventricular valvuloplasty was performed in 18 patients and ventricular cavity closure in 15 patients (29%). During a median follow-up of 2.4 years (interquartile range, 0.8-6.2), there was no mortality, cardiac arrests, heart transplants, or single ventricle palliation. The 15-year risk of reoperation and clinical ventricular tachycardia/fibrillation was 6.7% (95% CI, 0-14.3) and 2.4% (95% CI, 0-7.2), respectively. On latest imaging, pre- and postdebulking left ventricular ejection fraction did not significantly differ (P = .069), whereas no patients had signs of outflow tract obstruction, inflow tract obstruction, or moderate or greater atrioventricular valve regurgitation.
Conclusions: Large ventricular fibromas can be resected safely with appropriate surgical planning and an emphasis on debulking. Most children maintain left ventricular function and remain free of recurrent ventricular arrhythmias at follow-up. Extended follow-up is warranted to understand whether patients remain at risk for scar-based ventricular arrhythmias in the future.
期刊介绍:
The Journal of Thoracic and Cardiovascular Surgery presents original, peer-reviewed articles on diseases of the heart, great vessels, lungs and thorax with emphasis on surgical interventions. An official publication of The American Association for Thoracic Surgery and The Western Thoracic Surgical Association, the Journal focuses on techniques and developments in acquired cardiac surgery, congenital cardiac repair, thoracic procedures, heart and lung transplantation, mechanical circulatory support and other procedures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


