Yanmei Li, Xiaonan Feng, Na Chen, Shuhua Song, Min Yu, Yan Wang, Hongxia Zhang, Li Wang, Menghua Chen, Na Tian
{"title":"长期腹膜透析患者严重继发性甲状旁腺功能亢进症的预后和相关因素","authors":"Yanmei Li, Xiaonan Feng, Na Chen, Shuhua Song, Min Yu, Yan Wang, Hongxia Zhang, Li Wang, Menghua Chen, Na Tian","doi":"10.1080/0886022X.2024.2356022","DOIUrl":null,"url":null,"abstract":"<p><p>Secondary hyperparathyroidism (SHPT) can progress to severe SHPT (sSHPT), which affects the survival rate and quality of life of patients. This retrospective cohort study investigated risk factors for sSHPT and the association between SHPT and mortality (all-cause and infection-related) among 771 clinically stable patients (421 male patients; mean age, 51.2 years; median dialysis vintage, 28.3 months) who underwent >3 months of regular peritoneal dialysis (PD) between January 2013 and March 2021. The sSHPT and non-sSHPT groups comprised 75 (9.7%) (median progression, 35 months) and 696 patients, respectively. sSHPT was defined as a serum intact parathyroid hormone (PTH) level >800 pg/mL observed three times after active vitamin D pulse therapy. The influence of sSHPT on the prognosis of and risk factors for sSHPT progression were evaluated using logistic and Cox regression analyses. After adjusting for confounding factors, higher (each 100-pg/mL increase) baseline PTH levels (95% confidence interval (CI) 1.206-1.649, <i>p</i> < .001), longer (each 1-year increase) dialysis vintages (95% CI 1.013-1.060, <i>p</i> = .002), higher concomitant diabetes rates (95% CI 1.375-10.374, <i>p =</i> .010), and lower (each 1-absolute unit decrease) <i>Kt</i>/<i>V</i> values (95% CI 0.859-0.984, <i>p =</i> .015) were independent risk factors for progression to sSHPT in patients on PD. During follow-up, 211 deaths occurred (sSHPT group, <i>n</i> = 35; non-sSHPT group, <i>n</i> = 176). The sSHPT group had significantly higher infection-related mortality rates than the non-sSHPT group (12.0% vs. 4.3%; <i>p</i> < .05), and sSHPT was associated with increased infection-related mortality. In conclusion, patients with sSHPT are at higher risk for death and infection-related mortality than patients without sSHPT.</p>","PeriodicalId":20839,"journal":{"name":"Renal Failure","volume":"46 1","pages":"2356022"},"PeriodicalIF":3.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11136472/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognosis and factors related to severe secondary hyperparathyroidism in long-term peritoneal dialysis patients.\",\"authors\":\"Yanmei Li, Xiaonan Feng, Na Chen, Shuhua Song, Min Yu, Yan Wang, Hongxia Zhang, Li Wang, Menghua Chen, Na Tian\",\"doi\":\"10.1080/0886022X.2024.2356022\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Secondary hyperparathyroidism (SHPT) can progress to severe SHPT (sSHPT), which affects the survival rate and quality of life of patients. This retrospective cohort study investigated risk factors for sSHPT and the association between SHPT and mortality (all-cause and infection-related) among 771 clinically stable patients (421 male patients; mean age, 51.2 years; median dialysis vintage, 28.3 months) who underwent >3 months of regular peritoneal dialysis (PD) between January 2013 and March 2021. The sSHPT and non-sSHPT groups comprised 75 (9.7%) (median progression, 35 months) and 696 patients, respectively. sSHPT was defined as a serum intact parathyroid hormone (PTH) level >800 pg/mL observed three times after active vitamin D pulse therapy. The influence of sSHPT on the prognosis of and risk factors for sSHPT progression were evaluated using logistic and Cox regression analyses. After adjusting for confounding factors, higher (each 100-pg/mL increase) baseline PTH levels (95% confidence interval (CI) 1.206-1.649, <i>p</i> < .001), longer (each 1-year increase) dialysis vintages (95% CI 1.013-1.060, <i>p</i> = .002), higher concomitant diabetes rates (95% CI 1.375-10.374, <i>p =</i> .010), and lower (each 1-absolute unit decrease) <i>Kt</i>/<i>V</i> values (95% CI 0.859-0.984, <i>p =</i> .015) were independent risk factors for progression to sSHPT in patients on PD. During follow-up, 211 deaths occurred (sSHPT group, <i>n</i> = 35; non-sSHPT group, <i>n</i> = 176). The sSHPT group had significantly higher infection-related mortality rates than the non-sSHPT group (12.0% vs. 4.3%; <i>p</i> < .05), and sSHPT was associated with increased infection-related mortality. In conclusion, patients with sSHPT are at higher risk for death and infection-related mortality than patients without sSHPT.</p>\",\"PeriodicalId\":20839,\"journal\":{\"name\":\"Renal Failure\",\"volume\":\"46 1\",\"pages\":\"2356022\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11136472/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Renal Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/0886022X.2024.2356022\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Renal Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/0886022X.2024.2356022","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Prognosis and factors related to severe secondary hyperparathyroidism in long-term peritoneal dialysis patients.
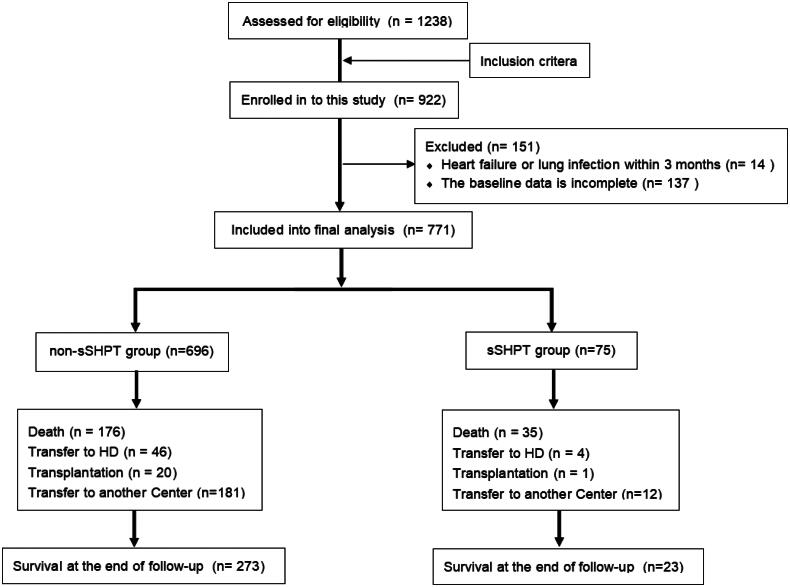
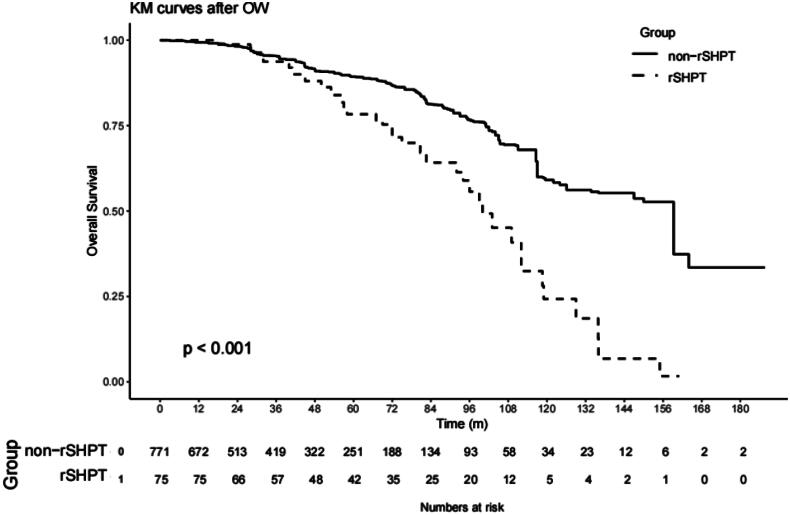
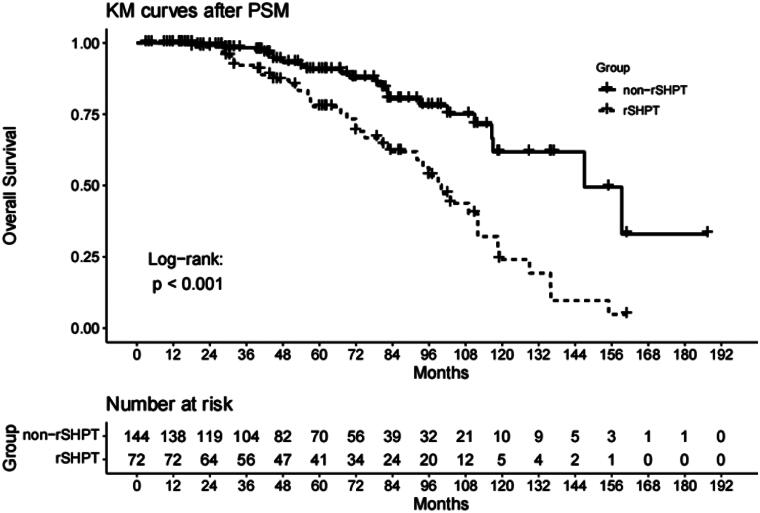
Secondary hyperparathyroidism (SHPT) can progress to severe SHPT (sSHPT), which affects the survival rate and quality of life of patients. This retrospective cohort study investigated risk factors for sSHPT and the association between SHPT and mortality (all-cause and infection-related) among 771 clinically stable patients (421 male patients; mean age, 51.2 years; median dialysis vintage, 28.3 months) who underwent >3 months of regular peritoneal dialysis (PD) between January 2013 and March 2021. The sSHPT and non-sSHPT groups comprised 75 (9.7%) (median progression, 35 months) and 696 patients, respectively. sSHPT was defined as a serum intact parathyroid hormone (PTH) level >800 pg/mL observed three times after active vitamin D pulse therapy. The influence of sSHPT on the prognosis of and risk factors for sSHPT progression were evaluated using logistic and Cox regression analyses. After adjusting for confounding factors, higher (each 100-pg/mL increase) baseline PTH levels (95% confidence interval (CI) 1.206-1.649, p < .001), longer (each 1-year increase) dialysis vintages (95% CI 1.013-1.060, p = .002), higher concomitant diabetes rates (95% CI 1.375-10.374, p = .010), and lower (each 1-absolute unit decrease) Kt/V values (95% CI 0.859-0.984, p = .015) were independent risk factors for progression to sSHPT in patients on PD. During follow-up, 211 deaths occurred (sSHPT group, n = 35; non-sSHPT group, n = 176). The sSHPT group had significantly higher infection-related mortality rates than the non-sSHPT group (12.0% vs. 4.3%; p < .05), and sSHPT was associated with increased infection-related mortality. In conclusion, patients with sSHPT are at higher risk for death and infection-related mortality than patients without sSHPT.
期刊介绍:
Renal Failure primarily concentrates on acute renal injury and its consequence, but also addresses advances in the fields of chronic renal failure, hypertension, and renal transplantation. Bringing together both clinical and experimental aspects of renal failure, this publication presents timely, practical information on pathology and pathophysiology of acute renal failure; nephrotoxicity of drugs and other substances; prevention, treatment, and therapy of renal failure; renal failure in association with transplantation, hypertension, and diabetes mellitus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


