Paolo Ghia, Carolyn Owen, John N. Allan, Jacqueline C. Barrientos, Paul M. Barr, Chunxue Shi, Anita Szoke, Christopher Abbazio, Gabriel S. Krigsfeld, Jan A. Burger
{"title":"慢性淋巴细胞白血病患者接受伊布替尼一线治疗后的总生存率与年龄匹配的普通人群相似:汇总事后分析","authors":"Paolo Ghia, Carolyn Owen, John N. Allan, Jacqueline C. Barrientos, Paul M. Barr, Chunxue Shi, Anita Szoke, Christopher Abbazio, Gabriel S. Krigsfeld, Jan A. Burger","doi":"10.1002/hem3.74","DOIUrl":null,"url":null,"abstract":"<p>Currently, there are no targeted agents that can cure chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), which is the most common leukemia among older adults.<span><sup>1</sup></span> In the absence of a curative regimen, the therapeutic goal is to maximize patients' life span while effectively managing disease symptoms.</p><p>Ibrutinib, a covalent, once-daily Bruton's tyrosine kinase inhibitor, has been shown to have survival superiority to chemotherapy (CT) and chemoimmunotherapy (CIT) in the first-line setting, including older adults and those with high-risk characteristics, and has demonstrated overall survival (OS) improvements in multiple pivotal trials.<span><sup>2-4</sup></span> In a long-term follow-up from RESONATE-2 of up to 8 years, first-line treatment with ibrutinib was associated with superior progression-free survival and OS compared with standard-of-care CT. Based on the results from the same study, adverse events (AEs) associated with ibrutinib can be managed effectively with dose reductions or dose holds, which results in AE resolution in most patients (85% and 90%, respectively), allowing them to remain on treatment and continue benefiting from ibrutinib.<span><sup>5</sup></span> The relatively long survival of patients with CLL/SLL treated with ibrutinib raises the question of whether the initiation of first-line ibrutinib could remove the survival hazard associated with CLL/SLL compared with the general population. The aims of this pooled analysis were to compare OS estimates of previously untreated patients with CLL/SLL who received ibrutinib or CT/CIT across three phase 3 studies with the OS estimates for an age-matched general population.</p><p>This post hoc analysis included data pooled from three randomized (1:1) controlled studies in patients with previously untreated CLL/SLL: RESONATE-2 (NCT01722487),<span><sup>2</sup></span> iLLUMINATE (NCT02264574),<span><sup>4</sup></span> and ECOG-ACRIN E1912 (NCT02048813).<span><sup>3</sup></span> Patients were separated into two groups: ibrutinib cohort (patients treated with ibrutinib, ibrutinib with rituximab, or ibrutinib with obinutuzumab); and CT/CIT cohort (patients receiving rituximab plus fludarabine plus cyclophosphamide, chlorambucil plus obinutuzumab, or single-agent chlorambucil). Details of the treatments and populations have been previously published for each study, and brief descriptions are included in the Supporting Information.</p><p>OS data from the time of initial CLL/SLL diagnosis for the ibrutinib-treated cohort or CT/CIT-treated cohort were compared with survival estimates for an age-matched US population in 2019 published by the Centers for Disease Control and Prevention (CDC).<span><sup>6</sup></span> Age-matched (1:1 match) simulated databases were generated based on the age distribution of patients treated with ibrutinib or CT/CIT from the three phase 3 clinical studies. OS probabilities were estimated using the Kaplan–Meier methodology. Safety data were evaluated for ibrutinib-based therapy from a pooled safety population consisting of patients from RESONATE-2 and iLLUMINATE. Participants in the ECOG-ACRIN E1912 study were excluded from safety assessments due to limitations in the details of AE data collection. Additional information about the study design and methods is included in the Supporting Information.</p><p>In the pooled sample from the three trials, 603 patients received first-line ibrutinib treatment and 424 received CT/CIT treatment (Table 1). The median age of patients in the ibrutinib-treated cohort at the time of randomization was 63 years. Most patients were men (65%), had an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 (57%), and had a Cumulative Illness Rating Scale (CIRS) score of ≤6 (80%). In the CT/CIT cohort, baseline characteristics were similar (median age at randomization, 67 years; men, 66%; ECOG performance status score of 0, 50%; CIRS score of ≤6, 76%). Other baseline clinical characteristics, including genetic testing results, are presented in Table 1.</p><p>In the ibrutinib-treated cohort, median treatment duration and median follow-up from the time of randomization were 39 months and 41 months, respectively; these times were 5 months and 40 months in the CT/CIT-treated cohort (Table S1). The median follow-up from the initial CLL/SLL diagnosis in the ibrutinib-treated cohort was 5.9 years.</p><p>OS for the full ibrutinib-treated cohort, calculated from the time of initial CLL/SLL diagnosis, was comparable to the OS estimate for the age-matched general population (hazard ratio [HR]; 95% confidence interval [CI] = 0.87 [0.63–1.19]). Twelve-year OS estimates (95% CI) were also similar between the full ibrutinib-treated cohort (82% [76–87]) and the age-matched general population (80% [76–83]) (Figure 1A). Similar OS estimates were observed between the ibrutinib cohort and the general population over a 12-year horizon in individuals aged <65 years and ≥65 years (Table S2 and Figure S1).</p><p>Conversely, OS was significantly lower (<i>p</i> = 0.05) for the CT/CIT cohort than for an aged-matched general population (HR [95% CI] = 1.35 [1.00–1.82]), with 12-year OS (95% CI) estimates of 69% (61–76) and 76% (72–80), respectively (Figure 1B).</p><p>Of the 248 evaluable patients from the RESONATE-2 and iLLUMINATE studies, 48 (19%) had dose reductions from a starting dose of 420 mg per day to manage AEs (Table S3). The median duration of ibrutinib treatment at a reduced dose was 31 months (range, 0–84+). Following ibrutinib dose reduction, 44 of 48 patients (92%) had resolution of the initial AE, and for 32 of 48 patients (67%), AEs either did not recur or recurred at a lower grade.</p><p>After experiencing AEs for which a dose reduction is recommended in the recently updated US Prescribing Information, 21 of 248 patients (9%) had dose reductions (Table S4).<span><sup>7</sup></span> Of those, 20 of 21 patients (95%) had resolution of the initial AE, and for 16 of 21 patients (76%), AEs either did not recur or recurred at a lower grade.</p><p>Ibrutinib dose holds of ≥7 days was used for AE management in 143 of 248 patients (58%) (Table S5). Ibrutinib was restarted at 420 mg in 118 of 248 patients (48%), at 280 mg in 35 of 248 patients (14%), and at 140 mg in 15 of 248 patients (6%) after a dose hold of ≥7 days. The occurrence of AEs leading to dose reductions and dose holds of ≥7 days was the highest in the first 2 years following ibrutinib initiation and subsided in subsequent years (Figures S2A and S2B).</p><p>Since the introduction of targeted CLL/SLL therapies, ibrutinib has had significantly improved outcomes across a broad range of patients with CLL/SLL compared with the previous standard of care, which has been demonstrated in several randomized clinical trials.<span><sup>2, 3, 8-11</sup></span> Ibrutinib has the longest follow-up data available for Bruton's tyrosine kinase inhibitor therapies, which uniquely allows for the assessment of long-term efficacy and safety.</p><p>Maintaining patients on therapy appears to be critical for maximizing clinical outcomes, including prolonged survival, with some patients receiving therapy for up to 8 years. For most patients in the RESONATE-2 study, long-term continuous ibrutinib treatment was possible while managing associated side effects through active dose management.<span><sup>5</sup></span> In the same study, survival outcomes were similar between patients treated with ibrutinib with and without dose reduction.<span><sup>12</sup></span> Similarly, in this pooled analysis, most patients experienced AE resolution after dose reduction, enabling them to stay on ibrutinib treatment.</p><p>Treatment discontinuation due to AEs occurred at similar rates across the phase 3 trials of first-line ibrutinib in this pooled analysis: in RESONATE-2, 24%<span><sup>5</sup></span> of patients discontinued ibrutinib due to AEs; in iLLUMINATE, 16%<span><sup>13</sup></span>; and ECOG1912, 22%.<span><sup>14</sup></span></p><p>Overall, the safety findings from this analysis are aligned with the previously described safety profile of first-line ibrutinib and are consistent with the data from individual phase 3 trials.<span><sup>3, 4, 15</sup></span></p><p>The strengths of this study include a relatively large number of patients and the length of follow-up across the three pooled studies. One key limitation was that, because of data availability, pooled ibrutinib data and general population survival estimates were matched only for age and not for other individual patient characteristics. In addition, we did not separate patients treated with CT from those treated with CIT to maintain the original analysis approach from these trials.</p><p>In conclusion, this post hoc analysis suggests that unlike first-line CT/CIT treatment, first-line ibrutinib is associated with survival rates that are similar to those seen in the age-matched general population. First-line ibrutinib treatment could eliminate excess mortality risk associated with CLL/SLL diagnosis in both younger and older adult patients.</p><p>Paolo Ghia, John N. Allan, Christopher Abbazio, and Gabriel S. Krigsfeld conceptualized the study. Christopher Abbazio and Gabriel S. Krigsfeld designed the methodology. Chunxue Shi performed study validation and statistical analysis. Chunxue Shi, Gabriel S. Krigsfeld, and Christopher Abbazio interpreted data. Paolo Ghia, Carolyn Owen, John N. Allan, Jacqueline C. Barrientos, Paul M. Barr, and Jan A. Burger participated in data acquisition/collection. All authors participated in the writing and review of the manuscript.</p><p>P. G. reports fees for consulting and honoraria from AbbVie, AstraZeneca, BeiGene, Bristol Myers Squibb, Janssen, Loxo@Lilly, Merck Sharp & Dohme Corp., and Roche; and research funding from AbbVie, AstraZeneca, and Janssen; and is an editor for HemaSphere. C. O. reports honoraria from AbbVie, AstraZeneca, BeiGene, Gilead, Incyte, Janssen, Merck, and Roche. J. N. A. reports fees for consulting from AbbVie, ADC Therapeutics, AstraZeneca, BeiGene, Epizyme, Genentech, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; research funding from BeiGene, Celgene, Genentech, Janssen, and TG Therapeutics; and has served on the speakers' bureau for AbbVie, BeiGene, Janssen, and Pharmacyclics LLC, an AbbVie Company. J. C. B. reports honoraria from Janssen and fees for consulting from AbbVie, AstraZeneca, BeiGene, and MEI Pharma; and research funding from Oncternal Therapeutics, Pharmacyclics LLC, an AbbVie Company, and VelosBio/Merck. P. M. B. reports fees for consulting from AbbVie, AstraZeneca, Bristol Myers Squibb, Celgene, Genentech, Gilead, Janssen, MEI Pharma, Merck, MorphoSys, Seattle Genetics, and TG Therapeutics; and research funding from AstraZeneca and TG Therapeutics. C. S. reports no conflicts of interest. A. S. reports employment and stock ownership with AbbVie. C. A. reports employment with AbbVie and stock ownership with AbbVie and Bristol Myers Squibb. G. S. K. reports employment with AbbVie and Bristol Myers Squibb; stock ownership with AbbVie, Bristol Myers Squibb, Dynavax, Inovio, and Moderna; and travel and accommodation expenses from AbbVie and Bristol Myers Squibb. J. A. B. reports honoraria from Gilead, Janssen, Novartis, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; consulting fees from BeiGene, Gilead, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; research funding from AstraZeneca, BeiGene, and Pharmacyclics LLC, an AbbVie Company; served on the speakers' bureau for BeiGene, Gilead, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; and received travel and accommodation expenses from Gilead, Janssen, Novartis, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics.</p><p>This study was sponsored by Pharmacyclics LLC, an AbbVie Company.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 5","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.74","citationCount":"0","resultStr":"{\"title\":\"First-line ibrutinib treatment in patients with chronic lymphocytic leukemia is associated with overall survival rates similar to those of an age-matched general population: A pooled post hoc analysis\",\"authors\":\"Paolo Ghia, Carolyn Owen, John N. Allan, Jacqueline C. Barrientos, Paul M. Barr, Chunxue Shi, Anita Szoke, Christopher Abbazio, Gabriel S. Krigsfeld, Jan A. Burger\",\"doi\":\"10.1002/hem3.74\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Currently, there are no targeted agents that can cure chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), which is the most common leukemia among older adults.<span><sup>1</sup></span> In the absence of a curative regimen, the therapeutic goal is to maximize patients' life span while effectively managing disease symptoms.</p><p>Ibrutinib, a covalent, once-daily Bruton's tyrosine kinase inhibitor, has been shown to have survival superiority to chemotherapy (CT) and chemoimmunotherapy (CIT) in the first-line setting, including older adults and those with high-risk characteristics, and has demonstrated overall survival (OS) improvements in multiple pivotal trials.<span><sup>2-4</sup></span> In a long-term follow-up from RESONATE-2 of up to 8 years, first-line treatment with ibrutinib was associated with superior progression-free survival and OS compared with standard-of-care CT. Based on the results from the same study, adverse events (AEs) associated with ibrutinib can be managed effectively with dose reductions or dose holds, which results in AE resolution in most patients (85% and 90%, respectively), allowing them to remain on treatment and continue benefiting from ibrutinib.<span><sup>5</sup></span> The relatively long survival of patients with CLL/SLL treated with ibrutinib raises the question of whether the initiation of first-line ibrutinib could remove the survival hazard associated with CLL/SLL compared with the general population. The aims of this pooled analysis were to compare OS estimates of previously untreated patients with CLL/SLL who received ibrutinib or CT/CIT across three phase 3 studies with the OS estimates for an age-matched general population.</p><p>This post hoc analysis included data pooled from three randomized (1:1) controlled studies in patients with previously untreated CLL/SLL: RESONATE-2 (NCT01722487),<span><sup>2</sup></span> iLLUMINATE (NCT02264574),<span><sup>4</sup></span> and ECOG-ACRIN E1912 (NCT02048813).<span><sup>3</sup></span> Patients were separated into two groups: ibrutinib cohort (patients treated with ibrutinib, ibrutinib with rituximab, or ibrutinib with obinutuzumab); and CT/CIT cohort (patients receiving rituximab plus fludarabine plus cyclophosphamide, chlorambucil plus obinutuzumab, or single-agent chlorambucil). Details of the treatments and populations have been previously published for each study, and brief descriptions are included in the Supporting Information.</p><p>OS data from the time of initial CLL/SLL diagnosis for the ibrutinib-treated cohort or CT/CIT-treated cohort were compared with survival estimates for an age-matched US population in 2019 published by the Centers for Disease Control and Prevention (CDC).<span><sup>6</sup></span> Age-matched (1:1 match) simulated databases were generated based on the age distribution of patients treated with ibrutinib or CT/CIT from the three phase 3 clinical studies. OS probabilities were estimated using the Kaplan–Meier methodology. Safety data were evaluated for ibrutinib-based therapy from a pooled safety population consisting of patients from RESONATE-2 and iLLUMINATE. Participants in the ECOG-ACRIN E1912 study were excluded from safety assessments due to limitations in the details of AE data collection. Additional information about the study design and methods is included in the Supporting Information.</p><p>In the pooled sample from the three trials, 603 patients received first-line ibrutinib treatment and 424 received CT/CIT treatment (Table 1). The median age of patients in the ibrutinib-treated cohort at the time of randomization was 63 years. Most patients were men (65%), had an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 (57%), and had a Cumulative Illness Rating Scale (CIRS) score of ≤6 (80%). In the CT/CIT cohort, baseline characteristics were similar (median age at randomization, 67 years; men, 66%; ECOG performance status score of 0, 50%; CIRS score of ≤6, 76%). Other baseline clinical characteristics, including genetic testing results, are presented in Table 1.</p><p>In the ibrutinib-treated cohort, median treatment duration and median follow-up from the time of randomization were 39 months and 41 months, respectively; these times were 5 months and 40 months in the CT/CIT-treated cohort (Table S1). The median follow-up from the initial CLL/SLL diagnosis in the ibrutinib-treated cohort was 5.9 years.</p><p>OS for the full ibrutinib-treated cohort, calculated from the time of initial CLL/SLL diagnosis, was comparable to the OS estimate for the age-matched general population (hazard ratio [HR]; 95% confidence interval [CI] = 0.87 [0.63–1.19]). Twelve-year OS estimates (95% CI) were also similar between the full ibrutinib-treated cohort (82% [76–87]) and the age-matched general population (80% [76–83]) (Figure 1A). Similar OS estimates were observed between the ibrutinib cohort and the general population over a 12-year horizon in individuals aged <65 years and ≥65 years (Table S2 and Figure S1).</p><p>Conversely, OS was significantly lower (<i>p</i> = 0.05) for the CT/CIT cohort than for an aged-matched general population (HR [95% CI] = 1.35 [1.00–1.82]), with 12-year OS (95% CI) estimates of 69% (61–76) and 76% (72–80), respectively (Figure 1B).</p><p>Of the 248 evaluable patients from the RESONATE-2 and iLLUMINATE studies, 48 (19%) had dose reductions from a starting dose of 420 mg per day to manage AEs (Table S3). The median duration of ibrutinib treatment at a reduced dose was 31 months (range, 0–84+). Following ibrutinib dose reduction, 44 of 48 patients (92%) had resolution of the initial AE, and for 32 of 48 patients (67%), AEs either did not recur or recurred at a lower grade.</p><p>After experiencing AEs for which a dose reduction is recommended in the recently updated US Prescribing Information, 21 of 248 patients (9%) had dose reductions (Table S4).<span><sup>7</sup></span> Of those, 20 of 21 patients (95%) had resolution of the initial AE, and for 16 of 21 patients (76%), AEs either did not recur or recurred at a lower grade.</p><p>Ibrutinib dose holds of ≥7 days was used for AE management in 143 of 248 patients (58%) (Table S5). Ibrutinib was restarted at 420 mg in 118 of 248 patients (48%), at 280 mg in 35 of 248 patients (14%), and at 140 mg in 15 of 248 patients (6%) after a dose hold of ≥7 days. The occurrence of AEs leading to dose reductions and dose holds of ≥7 days was the highest in the first 2 years following ibrutinib initiation and subsided in subsequent years (Figures S2A and S2B).</p><p>Since the introduction of targeted CLL/SLL therapies, ibrutinib has had significantly improved outcomes across a broad range of patients with CLL/SLL compared with the previous standard of care, which has been demonstrated in several randomized clinical trials.<span><sup>2, 3, 8-11</sup></span> Ibrutinib has the longest follow-up data available for Bruton's tyrosine kinase inhibitor therapies, which uniquely allows for the assessment of long-term efficacy and safety.</p><p>Maintaining patients on therapy appears to be critical for maximizing clinical outcomes, including prolonged survival, with some patients receiving therapy for up to 8 years. For most patients in the RESONATE-2 study, long-term continuous ibrutinib treatment was possible while managing associated side effects through active dose management.<span><sup>5</sup></span> In the same study, survival outcomes were similar between patients treated with ibrutinib with and without dose reduction.<span><sup>12</sup></span> Similarly, in this pooled analysis, most patients experienced AE resolution after dose reduction, enabling them to stay on ibrutinib treatment.</p><p>Treatment discontinuation due to AEs occurred at similar rates across the phase 3 trials of first-line ibrutinib in this pooled analysis: in RESONATE-2, 24%<span><sup>5</sup></span> of patients discontinued ibrutinib due to AEs; in iLLUMINATE, 16%<span><sup>13</sup></span>; and ECOG1912, 22%.<span><sup>14</sup></span></p><p>Overall, the safety findings from this analysis are aligned with the previously described safety profile of first-line ibrutinib and are consistent with the data from individual phase 3 trials.<span><sup>3, 4, 15</sup></span></p><p>The strengths of this study include a relatively large number of patients and the length of follow-up across the three pooled studies. One key limitation was that, because of data availability, pooled ibrutinib data and general population survival estimates were matched only for age and not for other individual patient characteristics. In addition, we did not separate patients treated with CT from those treated with CIT to maintain the original analysis approach from these trials.</p><p>In conclusion, this post hoc analysis suggests that unlike first-line CT/CIT treatment, first-line ibrutinib is associated with survival rates that are similar to those seen in the age-matched general population. First-line ibrutinib treatment could eliminate excess mortality risk associated with CLL/SLL diagnosis in both younger and older adult patients.</p><p>Paolo Ghia, John N. Allan, Christopher Abbazio, and Gabriel S. Krigsfeld conceptualized the study. Christopher Abbazio and Gabriel S. Krigsfeld designed the methodology. Chunxue Shi performed study validation and statistical analysis. Chunxue Shi, Gabriel S. Krigsfeld, and Christopher Abbazio interpreted data. Paolo Ghia, Carolyn Owen, John N. Allan, Jacqueline C. Barrientos, Paul M. Barr, and Jan A. Burger participated in data acquisition/collection. All authors participated in the writing and review of the manuscript.</p><p>P. G. reports fees for consulting and honoraria from AbbVie, AstraZeneca, BeiGene, Bristol Myers Squibb, Janssen, Loxo@Lilly, Merck Sharp & Dohme Corp., and Roche; and research funding from AbbVie, AstraZeneca, and Janssen; and is an editor for HemaSphere. C. O. reports honoraria from AbbVie, AstraZeneca, BeiGene, Gilead, Incyte, Janssen, Merck, and Roche. J. N. A. reports fees for consulting from AbbVie, ADC Therapeutics, AstraZeneca, BeiGene, Epizyme, Genentech, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; research funding from BeiGene, Celgene, Genentech, Janssen, and TG Therapeutics; and has served on the speakers' bureau for AbbVie, BeiGene, Janssen, and Pharmacyclics LLC, an AbbVie Company. J. C. B. reports honoraria from Janssen and fees for consulting from AbbVie, AstraZeneca, BeiGene, and MEI Pharma; and research funding from Oncternal Therapeutics, Pharmacyclics LLC, an AbbVie Company, and VelosBio/Merck. P. M. B. reports fees for consulting from AbbVie, AstraZeneca, Bristol Myers Squibb, Celgene, Genentech, Gilead, Janssen, MEI Pharma, Merck, MorphoSys, Seattle Genetics, and TG Therapeutics; and research funding from AstraZeneca and TG Therapeutics. C. S. reports no conflicts of interest. A. S. reports employment and stock ownership with AbbVie. C. A. reports employment with AbbVie and stock ownership with AbbVie and Bristol Myers Squibb. G. S. K. reports employment with AbbVie and Bristol Myers Squibb; stock ownership with AbbVie, Bristol Myers Squibb, Dynavax, Inovio, and Moderna; and travel and accommodation expenses from AbbVie and Bristol Myers Squibb. J. A. B. reports honoraria from Gilead, Janssen, Novartis, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; consulting fees from BeiGene, Gilead, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; research funding from AstraZeneca, BeiGene, and Pharmacyclics LLC, an AbbVie Company; served on the speakers' bureau for BeiGene, Gilead, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; and received travel and accommodation expenses from Gilead, Janssen, Novartis, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics.</p><p>This study was sponsored by Pharmacyclics LLC, an AbbVie Company.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 5\",\"pages\":\"\"},\"PeriodicalIF\":14.6000,\"publicationDate\":\"2024-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.74\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.74\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.74","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
慢性淋巴细胞白血病/小淋巴细胞淋巴瘤(CLL/SLL)是老年人中最常见的白血病,目前还没有靶向药物可以治愈慢性淋巴细胞白血病/小淋巴细胞淋巴瘤。伊布替尼是一种共价、每日一次的布鲁顿酪氨酸激酶抑制剂,在一线治疗(包括老年人和高危人群)中,其生存期优于化疗(CT)和化学免疫疗法(CIT),并在多项关键性试验中证明其总生存期(OS)有所改善。在RESONATE-2长达8年的长期随访中,伊布替尼一线治疗的无进展生存期和OS均优于标准治疗CT。根据同一研究的结果,与伊布替尼相关的不良反应(AEs)可通过减少剂量或暂停剂量得到有效控制,从而使大多数患者(分别为 85% 和 90%)的不良反应得到缓解,使他们能够继续接受治疗并继续从伊布替尼中获益。这项汇总分析的目的是将三项三期研究中接受伊布替尼或CT/CIT治疗的既往未接受治疗的CLL/SLL患者的OS估计值与年龄匹配的普通人群的OS估计值进行比较。这项事后分析汇总了三项针对既往未接受过治疗的 CLL/SLL 患者的随机(1:1)对照研究数据:RESONATE-2 (NCT01722487)、2 iLLUMINATE (NCT02264574)4 和 ECOG-ACRIN E1912 (NCT02048813)。3 患者分为两组:伊布替尼队列(接受伊布替尼、伊布替尼联合利妥昔单抗或伊布替尼联合奥比妥珠单抗治疗的患者);CT/CIT队列(接受利妥昔单抗联合氟达拉滨联合环磷酰胺、氯布嘧啶联合奥比妥珠单抗或单药氯布嘧啶治疗的患者)。伊布替尼治疗队列或CT/CIT治疗队列自初次诊断CLL/SLL时的OS数据与美国疾病控制和预防中心(CDC)发布的2019年美国年龄匹配人群的生存估计值进行了比较。6 根据三项三期临床研究中接受伊布替尼或 CT/CIT 治疗的患者年龄分布生成了年龄匹配(1:1 匹配)的模拟数据库。采用 Kaplan-Meier 方法估算 OS 概率。对基于伊布替尼疗法的安全性数据进行了评估,该数据来自RESONATE-2和iLLUMINATE患者的集合安全性人群。由于AE数据收集细节的限制,ECOG-ACRIN E1912研究的参与者未纳入安全性评估。关于研究设计和方法的更多信息请参见佐证资料。在三项试验的汇总样本中,603名患者接受了伊布替尼一线治疗,424名患者接受了CT/CIT治疗(表1)。接受伊布替尼治疗的患者随机分组时的中位年龄为63岁。大多数患者为男性(65%),东部合作肿瘤学组(ECOG)表现状态评分为0(57%),累积病情评分量表(CIRS)评分≤6(80%)。CT/CIT队列的基线特征相似(随机化时的中位年龄为67岁;男性占66%;ECOG表现状态评分为0分的占50%;CIRS评分≤6分的占76%)。表1列出了其他基线临床特征,包括基因检测结果。在伊布替尼治疗队列中,自随机化时起的中位治疗时间和中位随访时间分别为39个月和41个月;在CT/CIT治疗队列中,这两个时间分别为5个月和40个月(表S1)。伊布替尼治疗队列从最初诊断出CLL/SLL开始的中位随访时间为5.9年。伊布替尼治疗队列从最初诊断出CLL/SLL开始计算的OS与年龄匹配的普通人群的OS估计值相当(危险比[HR];95%置信区间[CI] = 0.87 [0.63-1.19])。伊布替尼治疗队列(82% [76-87])与年龄匹配的普通人群(80% [76-83])的12年OS估计值(95% CI)也相似(图1A)。相反,CT/CIT队列的OS显著低于(P = 0.05)年龄匹配的普通人群(HR [95% CI] = 1.35 [1.00-1. 在RESONATE-2和iLLUMINATE研究的248例可评估患者中,有48例(19%)从每天420毫克的起始剂量开始减少剂量以控制AEs(表S3)。伊布替尼减量治疗的中位持续时间为31个月(范围:0-84+)。减少伊布替尼剂量后,48 例患者中有 44 例(92%)的初始 AE 消失,48 例患者中有 32 例(67%)的 AE 不再复发或以较低的等级复发。在出现最近更新的美国处方信息中建议减少剂量的 AE 后,248 例患者中有 21 例(9%)减少了剂量(表 S4)。7其中,21例患者中有20例(95%)的初始AE得到缓解,21例患者中有16例(76%)的AE没有复发或复发等级较低。248例患者中有143例(58%)的AE处理采用了伊布替尼剂量暂停≥7天的方法(表S5)。248例患者中有118例(48%)在剂量维持≥7天后重新开始服用伊布替尼,剂量为420毫克;248例患者中有35例(14%)重新开始服用伊布替尼,剂量为280毫克;248例患者中有15例(6%)重新开始服用伊布替尼,剂量为140毫克。导致减量和停药≥7 天的 AEs 发生率在伊布替尼开始治疗后的头 2 年最高,随后几年有所下降(图 S2A 和 S2B)。自从引入 CLL/SLL 靶向疗法以来,与之前的标准疗法相比,伊布替尼显著改善了广大 CLL/SLL 患者的治疗效果,这已在多项随机临床试验中得到证实、3、8-11 在布鲁顿的酪氨酸激酶抑制剂疗法中,伊布替尼的随访时间最长,这为评估长期疗效和安全性提供了独特的条件。维持患者的治疗似乎对最大限度地提高临床疗效(包括延长生存期)至关重要,有些患者接受治疗的时间长达 8 年。对于RESONATE-2研究中的大多数患者来说,长期持续接受伊布替尼治疗是可能的,同时还可以通过积极的剂量管理来控制相关副作用。同样,在本汇总分析中,大多数患者在减量后 AE 消失,从而能够继续接受伊布替尼治疗。在本汇总分析中,伊布替尼一线 3 期试验中因 AE 而中断治疗的比例相似:在 RESONATE-2 中,24%5 的患者因 AE 而中断伊布替尼治疗;在 iLLUMINATE 中,16%13 的患者因 AE 而中断治疗;在 ECOG1912 中,22%的患者因 AE 而中断治疗。14 总体而言,该分析的安全性结果与之前描述的伊布替尼一线治疗的安全性特征一致,也与个别 3 期试验的数据一致、4、15 本研究的优点包括患者人数相对较多以及三项合并研究的随访时间较长。一项关键的局限性在于,由于数据的可用性,伊布替尼的汇总数据与普通人群的生存率估计值仅在年龄上进行了匹配,而未在其他患者个体特征上进行匹配。总之,这项事后分析表明,与一线CT/CIT治疗不同,一线伊布替尼的生存率与年龄匹配的普通人群的生存率相似。保罗-吉亚、约翰-N-阿兰、克里斯托弗-阿巴齐奥和加布里埃尔-S-克里格斯菲尔德构思了这项研究。Christopher Abbazio和Gabriel S. Krigsfeld设计了研究方法。施春雪进行了研究验证和统计分析。施春雪、加布里埃尔-S-克里格斯菲尔德和克里斯托弗-阿巴齐奥解释数据。Paolo Ghia、Carolyn Owen、John N. Allan、Jacqueline C. Barrientos、Paul M. Barr 和 Jan A. Burger 参与了数据采集/收集工作。所有作者都参与了稿件的撰写和审阅。P. G.从艾伯维、阿斯利康、BeiGene、百时美施贵宝、杨森、Loxo@Lilly、默沙东和罗氏公司领取咨询费和酬金;从艾伯维、阿斯利康和杨森公司领取研究经费;并且是 HemaSphere 的编辑。C. O.报告了来自艾伯维、阿斯利康、BeiGene、吉利德、Incyte、杨森、默克和罗氏的酬金。J. N. A.报告了来自艾伯维、ADC Therapeutics、阿斯利康、BeiGene、Epizyme、基因泰克、杨森、艾伯维公司旗下的 Pharmacyclics LLC 和 TG Therapeutics 的咨询费;来自 BeiGene、Celgene、基因泰克、杨森和 TG Therapeutics 的研究经费;并曾担任艾伯维、BeiGene、杨森和艾伯维公司旗下的 Pharmacyclics LLC 的发言人。J. C. B. 报告了杨森公司的酬金以及艾伯维、阿斯利康、BeiGene 和 MEI Pharma 的咨询费;以及 Oncternal Therapeutics、艾伯维旗下 Pharmacyclics LLC 和 VelosBio/Merck 的研究经费。P. M. B. 报告从艾伯维、阿斯利康、百时美施贵宝、Celgene、基因泰克、吉利德、杨森、MEI Pharma、默克、MorphoSys、西雅图基因公司和 TG Therapeutics 获得咨询费;从阿斯利康和 TG Therapeutics 获得研究经费。C. S. 报告没有利益冲突。A. S. 报告在艾伯维公司任职并持有股票。C. A. 报告受雇于艾伯维公司,并持有艾伯维公司和百时美施贵宝公司的股票。G. S. K. 报告受雇于艾伯维公司和百时美施贵宝公司;持有艾伯维公司、百时美施贵宝公司、Dynavax、Inovio 和 Moderna 的股票;以及艾伯维公司和百时美施贵宝公司提供的差旅和住宿费用。J. A. B.报告了来自吉利德、杨森、诺华、Pharmacyclics LLC、艾伯维公司和 TG Therapeutics 的酬金;来自 BeiGene、吉利德、杨森、Pharmacyclics LLC、艾伯维公司和 TG Therapeutics 的咨询费;来自阿斯利康、BeiGene 和艾伯维公司旗下 Pharmacyclics LLC 的研究经费;担任 BeiGene、吉利德、杨森、艾伯维公司旗下 Pharmacyclics LLC 和 TG Therapeutics 的发言人;并从吉利德、杨森、诺华、艾伯维公司旗下 Pharmacyclics LLC 和 TG Therapeutics 处获得差旅和住宿费用。本研究由艾伯维公司旗下的 Pharmacyclics LLC 赞助。
First-line ibrutinib treatment in patients with chronic lymphocytic leukemia is associated with overall survival rates similar to those of an age-matched general population: A pooled post hoc analysis
Currently, there are no targeted agents that can cure chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), which is the most common leukemia among older adults.1 In the absence of a curative regimen, the therapeutic goal is to maximize patients' life span while effectively managing disease symptoms.
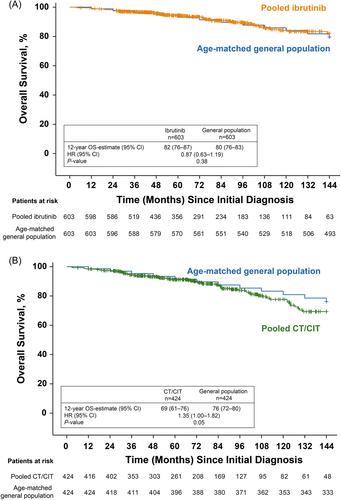
Ibrutinib, a covalent, once-daily Bruton's tyrosine kinase inhibitor, has been shown to have survival superiority to chemotherapy (CT) and chemoimmunotherapy (CIT) in the first-line setting, including older adults and those with high-risk characteristics, and has demonstrated overall survival (OS) improvements in multiple pivotal trials.2-4 In a long-term follow-up from RESONATE-2 of up to 8 years, first-line treatment with ibrutinib was associated with superior progression-free survival and OS compared with standard-of-care CT. Based on the results from the same study, adverse events (AEs) associated with ibrutinib can be managed effectively with dose reductions or dose holds, which results in AE resolution in most patients (85% and 90%, respectively), allowing them to remain on treatment and continue benefiting from ibrutinib.5 The relatively long survival of patients with CLL/SLL treated with ibrutinib raises the question of whether the initiation of first-line ibrutinib could remove the survival hazard associated with CLL/SLL compared with the general population. The aims of this pooled analysis were to compare OS estimates of previously untreated patients with CLL/SLL who received ibrutinib or CT/CIT across three phase 3 studies with the OS estimates for an age-matched general population.
This post hoc analysis included data pooled from three randomized (1:1) controlled studies in patients with previously untreated CLL/SLL: RESONATE-2 (NCT01722487),2 iLLUMINATE (NCT02264574),4 and ECOG-ACRIN E1912 (NCT02048813).3 Patients were separated into two groups: ibrutinib cohort (patients treated with ibrutinib, ibrutinib with rituximab, or ibrutinib with obinutuzumab); and CT/CIT cohort (patients receiving rituximab plus fludarabine plus cyclophosphamide, chlorambucil plus obinutuzumab, or single-agent chlorambucil). Details of the treatments and populations have been previously published for each study, and brief descriptions are included in the Supporting Information.
OS data from the time of initial CLL/SLL diagnosis for the ibrutinib-treated cohort or CT/CIT-treated cohort were compared with survival estimates for an age-matched US population in 2019 published by the Centers for Disease Control and Prevention (CDC).6 Age-matched (1:1 match) simulated databases were generated based on the age distribution of patients treated with ibrutinib or CT/CIT from the three phase 3 clinical studies. OS probabilities were estimated using the Kaplan–Meier methodology. Safety data were evaluated for ibrutinib-based therapy from a pooled safety population consisting of patients from RESONATE-2 and iLLUMINATE. Participants in the ECOG-ACRIN E1912 study were excluded from safety assessments due to limitations in the details of AE data collection. Additional information about the study design and methods is included in the Supporting Information.
In the pooled sample from the three trials, 603 patients received first-line ibrutinib treatment and 424 received CT/CIT treatment (Table 1). The median age of patients in the ibrutinib-treated cohort at the time of randomization was 63 years. Most patients were men (65%), had an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 (57%), and had a Cumulative Illness Rating Scale (CIRS) score of ≤6 (80%). In the CT/CIT cohort, baseline characteristics were similar (median age at randomization, 67 years; men, 66%; ECOG performance status score of 0, 50%; CIRS score of ≤6, 76%). Other baseline clinical characteristics, including genetic testing results, are presented in Table 1.
In the ibrutinib-treated cohort, median treatment duration and median follow-up from the time of randomization were 39 months and 41 months, respectively; these times were 5 months and 40 months in the CT/CIT-treated cohort (Table S1). The median follow-up from the initial CLL/SLL diagnosis in the ibrutinib-treated cohort was 5.9 years.
OS for the full ibrutinib-treated cohort, calculated from the time of initial CLL/SLL diagnosis, was comparable to the OS estimate for the age-matched general population (hazard ratio [HR]; 95% confidence interval [CI] = 0.87 [0.63–1.19]). Twelve-year OS estimates (95% CI) were also similar between the full ibrutinib-treated cohort (82% [76–87]) and the age-matched general population (80% [76–83]) (Figure 1A). Similar OS estimates were observed between the ibrutinib cohort and the general population over a 12-year horizon in individuals aged <65 years and ≥65 years (Table S2 and Figure S1).
Conversely, OS was significantly lower (p = 0.05) for the CT/CIT cohort than for an aged-matched general population (HR [95% CI] = 1.35 [1.00–1.82]), with 12-year OS (95% CI) estimates of 69% (61–76) and 76% (72–80), respectively (Figure 1B).
Of the 248 evaluable patients from the RESONATE-2 and iLLUMINATE studies, 48 (19%) had dose reductions from a starting dose of 420 mg per day to manage AEs (Table S3). The median duration of ibrutinib treatment at a reduced dose was 31 months (range, 0–84+). Following ibrutinib dose reduction, 44 of 48 patients (92%) had resolution of the initial AE, and for 32 of 48 patients (67%), AEs either did not recur or recurred at a lower grade.
After experiencing AEs for which a dose reduction is recommended in the recently updated US Prescribing Information, 21 of 248 patients (9%) had dose reductions (Table S4).7 Of those, 20 of 21 patients (95%) had resolution of the initial AE, and for 16 of 21 patients (76%), AEs either did not recur or recurred at a lower grade.
Ibrutinib dose holds of ≥7 days was used for AE management in 143 of 248 patients (58%) (Table S5). Ibrutinib was restarted at 420 mg in 118 of 248 patients (48%), at 280 mg in 35 of 248 patients (14%), and at 140 mg in 15 of 248 patients (6%) after a dose hold of ≥7 days. The occurrence of AEs leading to dose reductions and dose holds of ≥7 days was the highest in the first 2 years following ibrutinib initiation and subsided in subsequent years (Figures S2A and S2B).
Since the introduction of targeted CLL/SLL therapies, ibrutinib has had significantly improved outcomes across a broad range of patients with CLL/SLL compared with the previous standard of care, which has been demonstrated in several randomized clinical trials.2, 3, 8-11 Ibrutinib has the longest follow-up data available for Bruton's tyrosine kinase inhibitor therapies, which uniquely allows for the assessment of long-term efficacy and safety.
Maintaining patients on therapy appears to be critical for maximizing clinical outcomes, including prolonged survival, with some patients receiving therapy for up to 8 years. For most patients in the RESONATE-2 study, long-term continuous ibrutinib treatment was possible while managing associated side effects through active dose management.5 In the same study, survival outcomes were similar between patients treated with ibrutinib with and without dose reduction.12 Similarly, in this pooled analysis, most patients experienced AE resolution after dose reduction, enabling them to stay on ibrutinib treatment.
Treatment discontinuation due to AEs occurred at similar rates across the phase 3 trials of first-line ibrutinib in this pooled analysis: in RESONATE-2, 24%5 of patients discontinued ibrutinib due to AEs; in iLLUMINATE, 16%13; and ECOG1912, 22%.14
Overall, the safety findings from this analysis are aligned with the previously described safety profile of first-line ibrutinib and are consistent with the data from individual phase 3 trials.3, 4, 15
The strengths of this study include a relatively large number of patients and the length of follow-up across the three pooled studies. One key limitation was that, because of data availability, pooled ibrutinib data and general population survival estimates were matched only for age and not for other individual patient characteristics. In addition, we did not separate patients treated with CT from those treated with CIT to maintain the original analysis approach from these trials.
In conclusion, this post hoc analysis suggests that unlike first-line CT/CIT treatment, first-line ibrutinib is associated with survival rates that are similar to those seen in the age-matched general population. First-line ibrutinib treatment could eliminate excess mortality risk associated with CLL/SLL diagnosis in both younger and older adult patients.
Paolo Ghia, John N. Allan, Christopher Abbazio, and Gabriel S. Krigsfeld conceptualized the study. Christopher Abbazio and Gabriel S. Krigsfeld designed the methodology. Chunxue Shi performed study validation and statistical analysis. Chunxue Shi, Gabriel S. Krigsfeld, and Christopher Abbazio interpreted data. Paolo Ghia, Carolyn Owen, John N. Allan, Jacqueline C. Barrientos, Paul M. Barr, and Jan A. Burger participated in data acquisition/collection. All authors participated in the writing and review of the manuscript.
P. G. reports fees for consulting and honoraria from AbbVie, AstraZeneca, BeiGene, Bristol Myers Squibb, Janssen, Loxo@Lilly, Merck Sharp & Dohme Corp., and Roche; and research funding from AbbVie, AstraZeneca, and Janssen; and is an editor for HemaSphere. C. O. reports honoraria from AbbVie, AstraZeneca, BeiGene, Gilead, Incyte, Janssen, Merck, and Roche. J. N. A. reports fees for consulting from AbbVie, ADC Therapeutics, AstraZeneca, BeiGene, Epizyme, Genentech, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; research funding from BeiGene, Celgene, Genentech, Janssen, and TG Therapeutics; and has served on the speakers' bureau for AbbVie, BeiGene, Janssen, and Pharmacyclics LLC, an AbbVie Company. J. C. B. reports honoraria from Janssen and fees for consulting from AbbVie, AstraZeneca, BeiGene, and MEI Pharma; and research funding from Oncternal Therapeutics, Pharmacyclics LLC, an AbbVie Company, and VelosBio/Merck. P. M. B. reports fees for consulting from AbbVie, AstraZeneca, Bristol Myers Squibb, Celgene, Genentech, Gilead, Janssen, MEI Pharma, Merck, MorphoSys, Seattle Genetics, and TG Therapeutics; and research funding from AstraZeneca and TG Therapeutics. C. S. reports no conflicts of interest. A. S. reports employment and stock ownership with AbbVie. C. A. reports employment with AbbVie and stock ownership with AbbVie and Bristol Myers Squibb. G. S. K. reports employment with AbbVie and Bristol Myers Squibb; stock ownership with AbbVie, Bristol Myers Squibb, Dynavax, Inovio, and Moderna; and travel and accommodation expenses from AbbVie and Bristol Myers Squibb. J. A. B. reports honoraria from Gilead, Janssen, Novartis, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; consulting fees from BeiGene, Gilead, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; research funding from AstraZeneca, BeiGene, and Pharmacyclics LLC, an AbbVie Company; served on the speakers' bureau for BeiGene, Gilead, Janssen, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics; and received travel and accommodation expenses from Gilead, Janssen, Novartis, Pharmacyclics LLC, an AbbVie Company, and TG Therapeutics.
This study was sponsored by Pharmacyclics LLC, an AbbVie Company.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


