Nameer van Oosterom BPharm (Hon), PhD, Michael Barras PhD, Neil Cottrell PhD
{"title":"澳大利亚医院全髋关节和膝关节置换术后的静脉血栓栓塞预防:我们在用什么?","authors":"Nameer van Oosterom BPharm (Hon), PhD, Michael Barras PhD, Neil Cottrell PhD","doi":"10.1002/jppr.1919","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Venous thromboembolism (VTE) is a leading cause of preventable morbidity and mortality, with total hip arthroplasty (THA) and total knee arthroplasty (TKA) at the highest risk. Safe and appropriate thromboprophylaxis is essential. However, investigations into prescribing practices have been limited.</p>\n </section>\n \n <section>\n \n <h3> Aim</h3>\n \n <p>To describe current VTE prophylaxis regimens in Australian patients following an elective THA/TKA and compare these regimens to an international standard.</p>\n </section>\n \n <section>\n \n <h3> Method</h3>\n \n <p>A retrospective multisite case series of patients admitted for a THA/TKA in six tertiary hospitals in Queensland, Australia, was conducted over 12 months (1 October 2017–30 September 2018). Patient and medication data were collected following surgery and for 60 days after discharge to determine changes to the patients' thromboprophylaxis regimen. Results were summarised and compared to National Institute for Health and Care Excellence (NICE) guidelines. Ethical approval was granted by the Metro South Human Research Ethics Committee (Reference no: HREC/2018/QMD/46757) and the study conforms to the <i>National Statement on Ethical Conduct in Human Research</i>.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The study included 1011 patients (43.1% THA, 56.9% TKA), and thromboprophylaxis was used in 98.1% of inpatients and in 94.3% of discharge patients for 5.2 (±5.2) and 29.2 (±15.9) days (±standard deviation) respectively. Low-molecular-weight heparins (LMWHs) were the primary drugs for inpatients (71.2%) and aspirin 150 mg for discharge (42.0%), most commonly for 6 weeks (31.8%). Aspirin was used for significantly longer duration than rivaroxaban and LMWH (p < 0.001). A two-staged prophylaxis regimen was implemented, most commonly any anticoagulant as an inpatient; followed by rivaroxaban on discharge (32.7%) or an anticoagulant as an inpatient with aspirin on discharge (26.4%). Overall, adherence to NICE guidelines was low; THA: 8.7%, TKA: 5.9%.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>VTE prophylaxis regimens varied considerably, and consequently, adherence to international guidelines was low. There is a need for local, peer-led guidelines to ensure consistent, safe, and effective prophylaxis.</p>\n </section>\n </div>","PeriodicalId":16795,"journal":{"name":"Journal of Pharmacy Practice and Research","volume":"54 4","pages":"287-295"},"PeriodicalIF":1.0000,"publicationDate":"2024-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jppr.1919","citationCount":"0","resultStr":"{\"title\":\"Prevention of venous thromboembolism after total hip and knee arthroplasties in Australian hospitals: what are we using?\",\"authors\":\"Nameer van Oosterom BPharm (Hon), PhD, Michael Barras PhD, Neil Cottrell PhD\",\"doi\":\"10.1002/jppr.1919\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Venous thromboembolism (VTE) is a leading cause of preventable morbidity and mortality, with total hip arthroplasty (THA) and total knee arthroplasty (TKA) at the highest risk. Safe and appropriate thromboprophylaxis is essential. However, investigations into prescribing practices have been limited.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>To describe current VTE prophylaxis regimens in Australian patients following an elective THA/TKA and compare these regimens to an international standard.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Method</h3>\\n \\n <p>A retrospective multisite case series of patients admitted for a THA/TKA in six tertiary hospitals in Queensland, Australia, was conducted over 12 months (1 October 2017–30 September 2018). Patient and medication data were collected following surgery and for 60 days after discharge to determine changes to the patients' thromboprophylaxis regimen. Results were summarised and compared to National Institute for Health and Care Excellence (NICE) guidelines. Ethical approval was granted by the Metro South Human Research Ethics Committee (Reference no: HREC/2018/QMD/46757) and the study conforms to the <i>National Statement on Ethical Conduct in Human Research</i>.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The study included 1011 patients (43.1% THA, 56.9% TKA), and thromboprophylaxis was used in 98.1% of inpatients and in 94.3% of discharge patients for 5.2 (±5.2) and 29.2 (±15.9) days (±standard deviation) respectively. Low-molecular-weight heparins (LMWHs) were the primary drugs for inpatients (71.2%) and aspirin 150 mg for discharge (42.0%), most commonly for 6 weeks (31.8%). Aspirin was used for significantly longer duration than rivaroxaban and LMWH (p < 0.001). A two-staged prophylaxis regimen was implemented, most commonly any anticoagulant as an inpatient; followed by rivaroxaban on discharge (32.7%) or an anticoagulant as an inpatient with aspirin on discharge (26.4%). Overall, adherence to NICE guidelines was low; THA: 8.7%, TKA: 5.9%.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>VTE prophylaxis regimens varied considerably, and consequently, adherence to international guidelines was low. There is a need for local, peer-led guidelines to ensure consistent, safe, and effective prophylaxis.</p>\\n </section>\\n </div>\",\"PeriodicalId\":16795,\"journal\":{\"name\":\"Journal of Pharmacy Practice and Research\",\"volume\":\"54 4\",\"pages\":\"287-295\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-05-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jppr.1919\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmacy Practice and Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jppr.1919\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmacy Practice and Research","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jppr.1919","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Prevention of venous thromboembolism after total hip and knee arthroplasties in Australian hospitals: what are we using?
Background
Venous thromboembolism (VTE) is a leading cause of preventable morbidity and mortality, with total hip arthroplasty (THA) and total knee arthroplasty (TKA) at the highest risk. Safe and appropriate thromboprophylaxis is essential. However, investigations into prescribing practices have been limited.
Aim
To describe current VTE prophylaxis regimens in Australian patients following an elective THA/TKA and compare these regimens to an international standard.
Method
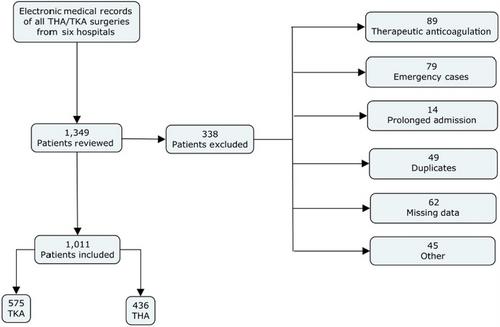
A retrospective multisite case series of patients admitted for a THA/TKA in six tertiary hospitals in Queensland, Australia, was conducted over 12 months (1 October 2017–30 September 2018). Patient and medication data were collected following surgery and for 60 days after discharge to determine changes to the patients' thromboprophylaxis regimen. Results were summarised and compared to National Institute for Health and Care Excellence (NICE) guidelines. Ethical approval was granted by the Metro South Human Research Ethics Committee (Reference no: HREC/2018/QMD/46757) and the study conforms to the National Statement on Ethical Conduct in Human Research.
Results
The study included 1011 patients (43.1% THA, 56.9% TKA), and thromboprophylaxis was used in 98.1% of inpatients and in 94.3% of discharge patients for 5.2 (±5.2) and 29.2 (±15.9) days (±standard deviation) respectively. Low-molecular-weight heparins (LMWHs) were the primary drugs for inpatients (71.2%) and aspirin 150 mg for discharge (42.0%), most commonly for 6 weeks (31.8%). Aspirin was used for significantly longer duration than rivaroxaban and LMWH (p < 0.001). A two-staged prophylaxis regimen was implemented, most commonly any anticoagulant as an inpatient; followed by rivaroxaban on discharge (32.7%) or an anticoagulant as an inpatient with aspirin on discharge (26.4%). Overall, adherence to NICE guidelines was low; THA: 8.7%, TKA: 5.9%.
Conclusion
VTE prophylaxis regimens varied considerably, and consequently, adherence to international guidelines was low. There is a need for local, peer-led guidelines to ensure consistent, safe, and effective prophylaxis.
期刊介绍:
The purpose of this document is to describe the structure, function and operations of the Journal of Pharmacy Practice and Research, the official journal of the Society of Hospital Pharmacists of Australia (SHPA). It is owned, published by and copyrighted to SHPA. However, the Journal is to some extent unique within SHPA in that it ‘…has complete editorial freedom in terms of content and is not under the direction of the Society or its Council in such matters…’. This statement, originally based on a Role Statement for the Editor-in-Chief 1993, is also based on the definition of ‘editorial independence’ from the World Association of Medical Editors and adopted by the International Committee of Medical Journal Editors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


