{"title":"重症监护病房重症社区获得性肺炎和流感患者中的侵袭性肺曲霉菌病:一项回顾性队列研究。","authors":"Wei-Chun Lee, Che-Chia Chang, Meng-Chin Ho, Chieh-Mo Lin, Shaw-Woei Leu, Chin-Kuo Lin, Yu-Hung Fang, Shu-Yi Huang, Yu-Ching Lin, Min-Chun Chuang, Tsung-Ming Yang, Ming-Szu Hung, Yen-Li Chou, Ying-Huang Tsai, Meng-Jer Hsieh","doi":"10.1186/s41479-024-00129-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong>The prevalence, clinical characteristics, and outcomes of invasive pulmonary aspergillosis in patients with severe community-acquired pneumonia (CAP) in intensive care units remain underestimated because of the lack of a disease-recognition scheme and the inadequacy of diagnostic tests.</p><p><strong>Objectives: </strong>To identify the prevalence, risk factors, and outcomes of severe CAP complicated with invasive pulmonary aspergillosis (IPA) in intensive care units (ICUs).</p><p><strong>Methods: </strong>We conducted a retrospective cohort study including recruited 311 ICU-hospitalized patients with severe CAP without influenza or with influenza. Bronchoalveolar lavage fluid (BALF) samples were from all patients and subjected to mycological testing. Patients were categorized as having proven or probable Aspergillus infection using a modified form of the AspICU algorithm comprising clinical, radiological, and mycological criteria.</p><p><strong>Measurements and main results: </strong>Of the 252 patients with severe CAP and 59 influenza patients evaluated, 24 met the diagnostic criteria for proven or probable Aspergillus infection in the CAP group and 9 patients in the influenza group, giving estimated prevalence values of 9.5% and 15.3%, respectively. COPD and the use of inhaled corticosteroids were independent risk factors for IPA. IPA in patients with severe CAP was significantly associated with the duration of mechanical support, the length of ICU stay, and the 28-day mortality.</p><p><strong>Conclusions: </strong>An aggressive diagnostic approach for IPA patients with severe CAP and not only influenza or COVID-19 should be pursued. Further randomized controlled trials need to evaluate the timing, safety, and efficacy of antifungal therapy in reducing IPA incidence and improving clinical outcomes.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"16 1","pages":"10"},"PeriodicalIF":6.2000,"publicationDate":"2024-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11127357/pdf/","citationCount":"0","resultStr":"{\"title\":\"Invasive pulmonary aspergillosis among patients with severe community-acquired pneumonia and influenza in ICUs: a retrospective cohort study.\",\"authors\":\"Wei-Chun Lee, Che-Chia Chang, Meng-Chin Ho, Chieh-Mo Lin, Shaw-Woei Leu, Chin-Kuo Lin, Yu-Hung Fang, Shu-Yi Huang, Yu-Ching Lin, Min-Chun Chuang, Tsung-Ming Yang, Ming-Szu Hung, Yen-Li Chou, Ying-Huang Tsai, Meng-Jer Hsieh\",\"doi\":\"10.1186/s41479-024-00129-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Rationale: </strong>The prevalence, clinical characteristics, and outcomes of invasive pulmonary aspergillosis in patients with severe community-acquired pneumonia (CAP) in intensive care units remain underestimated because of the lack of a disease-recognition scheme and the inadequacy of diagnostic tests.</p><p><strong>Objectives: </strong>To identify the prevalence, risk factors, and outcomes of severe CAP complicated with invasive pulmonary aspergillosis (IPA) in intensive care units (ICUs).</p><p><strong>Methods: </strong>We conducted a retrospective cohort study including recruited 311 ICU-hospitalized patients with severe CAP without influenza or with influenza. Bronchoalveolar lavage fluid (BALF) samples were from all patients and subjected to mycological testing. Patients were categorized as having proven or probable Aspergillus infection using a modified form of the AspICU algorithm comprising clinical, radiological, and mycological criteria.</p><p><strong>Measurements and main results: </strong>Of the 252 patients with severe CAP and 59 influenza patients evaluated, 24 met the diagnostic criteria for proven or probable Aspergillus infection in the CAP group and 9 patients in the influenza group, giving estimated prevalence values of 9.5% and 15.3%, respectively. COPD and the use of inhaled corticosteroids were independent risk factors for IPA. IPA in patients with severe CAP was significantly associated with the duration of mechanical support, the length of ICU stay, and the 28-day mortality.</p><p><strong>Conclusions: </strong>An aggressive diagnostic approach for IPA patients with severe CAP and not only influenza or COVID-19 should be pursued. Further randomized controlled trials need to evaluate the timing, safety, and efficacy of antifungal therapy in reducing IPA incidence and improving clinical outcomes.</p>\",\"PeriodicalId\":45120,\"journal\":{\"name\":\"Pneumonia\",\"volume\":\"16 1\",\"pages\":\"10\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2024-05-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11127357/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pneumonia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41479-024-00129-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-024-00129-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
理由:由于缺乏疾病识别方案以及诊断测试的不足,重症监护病房重症社区获得性肺炎(CAP)患者中侵袭性肺曲霉菌病的发病率、临床特征和预后仍被低估:目的:确定重症监护病房(ICU)中并发侵袭性肺曲霉菌病(IPA)的重症CAP的发病率、风险因素和预后:我们进行了一项回顾性队列研究,共招募了 311 名重症监护病房住院的重症 CAP 患者,这些患者既没有患流感,也没有患流感。对所有患者的支气管肺泡灌洗液(BALF)样本进行了真菌学检测。采用改良版的 AspICU 算法(包括临床、放射学和霉菌学标准),将患者分为已证实或可能感染曲霉菌:在接受评估的 252 名重症 CAP 患者和 59 名流感患者中,CAP 组有 24 人符合证实或可能感染曲霉菌的诊断标准,流感组有 9 人,估计感染率分别为 9.5% 和 15.3%。慢性阻塞性肺病和吸入皮质类固醇是导致 IPA 的独立风险因素。重症CAP患者的IPA与机械支持的持续时间、重症监护室的住院时间和28天的死亡率有显著相关性:结论:对于患有重症 CAP 的 IPA 患者,应采取积极的诊断方法,而不仅仅是流感或 COVID-19。需要进一步开展随机对照试验,评估抗真菌治疗在降低 IPA 发病率和改善临床预后方面的时机、安全性和有效性。
Invasive pulmonary aspergillosis among patients with severe community-acquired pneumonia and influenza in ICUs: a retrospective cohort study.
Rationale: The prevalence, clinical characteristics, and outcomes of invasive pulmonary aspergillosis in patients with severe community-acquired pneumonia (CAP) in intensive care units remain underestimated because of the lack of a disease-recognition scheme and the inadequacy of diagnostic tests.
Objectives: To identify the prevalence, risk factors, and outcomes of severe CAP complicated with invasive pulmonary aspergillosis (IPA) in intensive care units (ICUs).
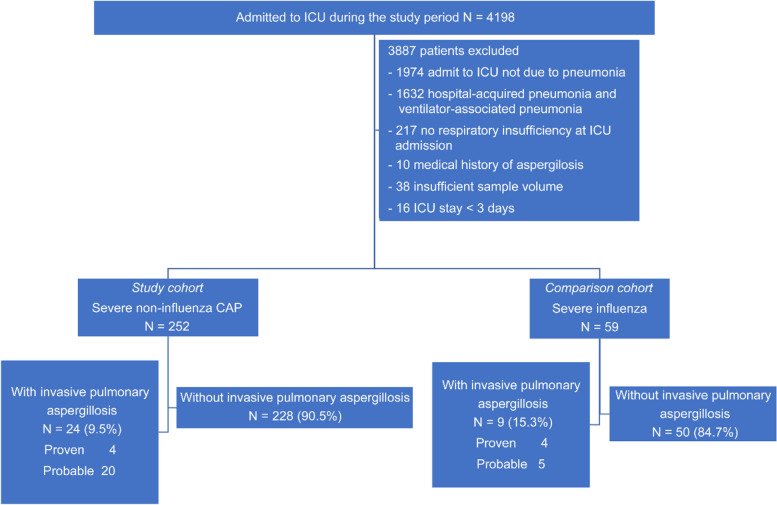
Methods: We conducted a retrospective cohort study including recruited 311 ICU-hospitalized patients with severe CAP without influenza or with influenza. Bronchoalveolar lavage fluid (BALF) samples were from all patients and subjected to mycological testing. Patients were categorized as having proven or probable Aspergillus infection using a modified form of the AspICU algorithm comprising clinical, radiological, and mycological criteria.
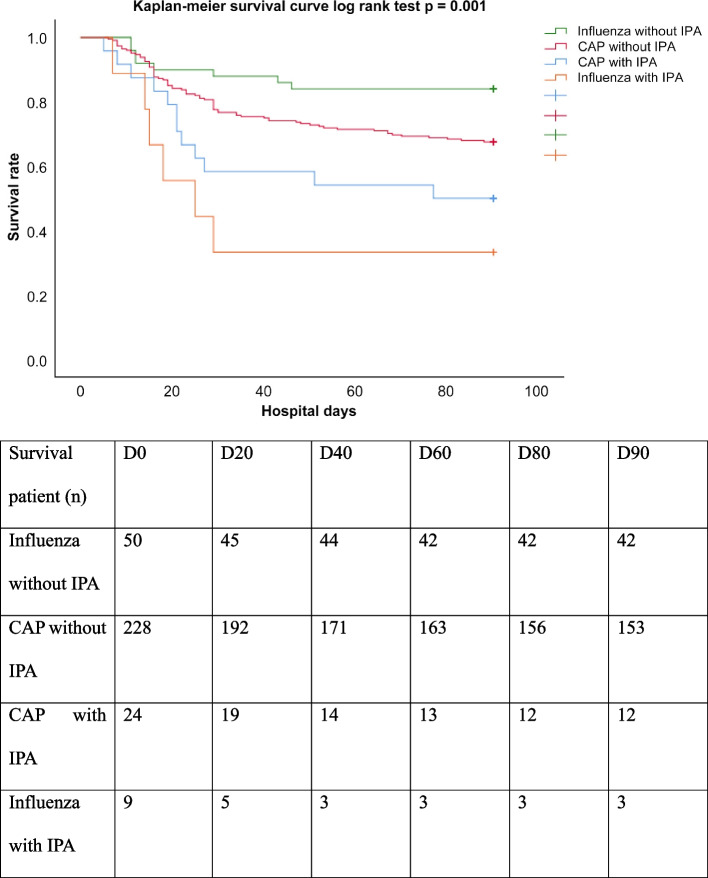
Measurements and main results: Of the 252 patients with severe CAP and 59 influenza patients evaluated, 24 met the diagnostic criteria for proven or probable Aspergillus infection in the CAP group and 9 patients in the influenza group, giving estimated prevalence values of 9.5% and 15.3%, respectively. COPD and the use of inhaled corticosteroids were independent risk factors for IPA. IPA in patients with severe CAP was significantly associated with the duration of mechanical support, the length of ICU stay, and the 28-day mortality.
Conclusions: An aggressive diagnostic approach for IPA patients with severe CAP and not only influenza or COVID-19 should be pursued. Further randomized controlled trials need to evaluate the timing, safety, and efficacy of antifungal therapy in reducing IPA incidence and improving clinical outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


