Susana Palao-Duarte, Dirk-Matthias Altenmüller, Christian Scheiwe, Anika Schinkel, Hansjörg Mast, Horst Urbach, Theo Demerath, Marius Schwabenland, Andreas Schulze-Bonhage, Kathrin Wagner, Marcel Heers
{"title":"电刺激图引导语言代表皮层癫痫相关肿瘤的个体化手术方法。","authors":"Susana Palao-Duarte, Dirk-Matthias Altenmüller, Christian Scheiwe, Anika Schinkel, Hansjörg Mast, Horst Urbach, Theo Demerath, Marius Schwabenland, Andreas Schulze-Bonhage, Kathrin Wagner, Marcel Heers","doi":"10.1002/epd2.20245","DOIUrl":null,"url":null,"abstract":"<p>In epilepsy patients with tumors involving the cortex with language representations, a comprehensive interdisciplinary workup is required to protect language function during surgical resection.<span><sup>1</sup></span></p><p>We report the presurgical evaluation of a patient with focal epilepsy due to a progressive tumor in the language area of the left temporal lobe. After non-invasive presurgical diagnostics, we performed an invasive subdural electroencephalogram (iEEG) with extraoperative electrical stimulation mapping (ESM) prior to tumor surgery.<span><sup>2</sup></span></p><p>A 22-year-old female university student with left-sided temporal lobe epilepsy was referred for invasive video-EEG monitoring and language mapping to guide resective tumor surgery. Her epilepsy began at the age of 20 years, and it was characterized by focal aware seizures with speech arrest, occasionally followed by focal impaired awareness seizures. Under monotherapy with Levetiracetam up to 4 g/day, she had two to three focal aware seizures/day, despite which she was able to finish her university studies. High-resolution 3T structural magnetic resonance imaging (s-MRI) showed a slowly progressive, partially contrast-enhancing low-grade neuroglial tumor located at the left posterior superior temporal gyrus (Figure 1, Panels A and B) and the basal insula. A functional language MRI (l-fMRI) confirmed left-hemispheric language dominance with activations directly adjacent to the tumor (Figure 1, Panel C). Presurgical neuropsychological assessment (NPS) revealed discrete word-finding difficulties, partly reduced verbal fluency and impaired verbal short-term and working memory performance. The right-handed patient had a normal physical examination. Written informed consent was obtained for the scientific publication of the patient's clinical data.</p><p>Invasive video-EEG monitoring for 4 days with a 32-contact subdural grid implanted over the left temporal lobe was performed (Figure 1, Panel D). The ESM language cortical mapping with 50 Hz (biphasic pulses, duration 250 μs, bipolar stimulation up to 15 mA, referential stimulation up to 18 mA) comprised six different language tasks as described in detail before.<span><sup>3</sup></span> Language representations were identified in contacts B2-3, B6, C5-C8, and D7 (Figure 1, Panel D). The language representation around contacts A3-4 and B4-5 could not be assessed due to unavoidable afterdischarges despite the additional use of lorazepam. In summary, the ESM showed a clear overlap of language representation and tumor in the left superior temporal gyrus. The irritative zone and the seizure onset zone overlapped with language representations (Figure 1, Panel D).</p><p>Due to the tumor's location, only the contrast-enhancing solid component and the cyst membrane could be resected via a transsylvian approach to minimize the risk of postoperative language deficits. No need for awake surgery with additional intraoperative language mapping was seen. The postsurgical NPS revealed unchanged performance, especially in language-related tasks, and no deterioration was found. The neuropathological diagnosis was a low-grade neuroepithelial tumor not elsewhere classified (IDH1, IDH2: wild-type; Multiplex Ligation-Dependent Probe Amplification: no BRAF-V600e mutation or BRAF-KIAA1549-fusion or homozygous CDKN2A/B loss, 850 k methylome analysis inconclusive). Postsurgical s-MRI showed no complications (Figure 1F). As it was impossible to resect the entire tumor and the seizure onset zone, it is likely that the patient will not become seizure-free after surgery.</p><p>The case presented illustrates how individualized concepts guide surgical decisions in patients with focal epilepsy due to a tumor in eloquent areas. The aim of removing the most relevant, contrast-enhancing tumor part was achieved without endangering cortical language representations based on solid ESM findings. It was necessary to prioritize avoiding damage to language areas over the complete removal of the tumor and the seizure onset area.</p><p>Robust functional assessment of language representations is critical to minimize the risk of permanent postoperative language deficits. The ESM is the gold standard method for accurately delineating the language-relevant cortex, although the procedure is not yet standardized.<span><sup>2-4</sup></span> As described by Wellmer et al., the type and number of applied language tasks vary between centers.<span><sup>3</sup></span> The l-fMRI allows visualization of hemispheric lateralization of language, but its localization value is not accurate enough to define the margins of surgical resection.<span><sup>4-6</sup></span> For a more rigorous evaluation before and after surgery, NPS assessment of language-associated functions is indispensable.<span><sup>7</sup></span></p><p>The evaluation of functional connectivity in iEEG is promising but has not yet been proven to be as accurate as ESM in iEEG.<span><sup>8</sup></span> Also, awake tumor surgery does not offer similar flexibility in choosing time windows free of afterdischarges and multimodal language tasks for comprehensive language mappings. So, ESM in iEEG remains the gold standard for guiding neurosurgical resection adjacent to cortical language representations.</p>","PeriodicalId":50508,"journal":{"name":"Epileptic Disorders","volume":"26 4","pages":"548-551"},"PeriodicalIF":1.9000,"publicationDate":"2024-05-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/epd2.20245","citationCount":"0","resultStr":"{\"title\":\"Electrical stimulation mapping guides individualized surgical approach in an epilepsy-associated tumor within language representing cortex\",\"authors\":\"Susana Palao-Duarte, Dirk-Matthias Altenmüller, Christian Scheiwe, Anika Schinkel, Hansjörg Mast, Horst Urbach, Theo Demerath, Marius Schwabenland, Andreas Schulze-Bonhage, Kathrin Wagner, Marcel Heers\",\"doi\":\"10.1002/epd2.20245\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In epilepsy patients with tumors involving the cortex with language representations, a comprehensive interdisciplinary workup is required to protect language function during surgical resection.<span><sup>1</sup></span></p><p>We report the presurgical evaluation of a patient with focal epilepsy due to a progressive tumor in the language area of the left temporal lobe. After non-invasive presurgical diagnostics, we performed an invasive subdural electroencephalogram (iEEG) with extraoperative electrical stimulation mapping (ESM) prior to tumor surgery.<span><sup>2</sup></span></p><p>A 22-year-old female university student with left-sided temporal lobe epilepsy was referred for invasive video-EEG monitoring and language mapping to guide resective tumor surgery. Her epilepsy began at the age of 20 years, and it was characterized by focal aware seizures with speech arrest, occasionally followed by focal impaired awareness seizures. Under monotherapy with Levetiracetam up to 4 g/day, she had two to three focal aware seizures/day, despite which she was able to finish her university studies. High-resolution 3T structural magnetic resonance imaging (s-MRI) showed a slowly progressive, partially contrast-enhancing low-grade neuroglial tumor located at the left posterior superior temporal gyrus (Figure 1, Panels A and B) and the basal insula. A functional language MRI (l-fMRI) confirmed left-hemispheric language dominance with activations directly adjacent to the tumor (Figure 1, Panel C). Presurgical neuropsychological assessment (NPS) revealed discrete word-finding difficulties, partly reduced verbal fluency and impaired verbal short-term and working memory performance. The right-handed patient had a normal physical examination. Written informed consent was obtained for the scientific publication of the patient's clinical data.</p><p>Invasive video-EEG monitoring for 4 days with a 32-contact subdural grid implanted over the left temporal lobe was performed (Figure 1, Panel D). The ESM language cortical mapping with 50 Hz (biphasic pulses, duration 250 μs, bipolar stimulation up to 15 mA, referential stimulation up to 18 mA) comprised six different language tasks as described in detail before.<span><sup>3</sup></span> Language representations were identified in contacts B2-3, B6, C5-C8, and D7 (Figure 1, Panel D). The language representation around contacts A3-4 and B4-5 could not be assessed due to unavoidable afterdischarges despite the additional use of lorazepam. In summary, the ESM showed a clear overlap of language representation and tumor in the left superior temporal gyrus. The irritative zone and the seizure onset zone overlapped with language representations (Figure 1, Panel D).</p><p>Due to the tumor's location, only the contrast-enhancing solid component and the cyst membrane could be resected via a transsylvian approach to minimize the risk of postoperative language deficits. No need for awake surgery with additional intraoperative language mapping was seen. The postsurgical NPS revealed unchanged performance, especially in language-related tasks, and no deterioration was found. The neuropathological diagnosis was a low-grade neuroepithelial tumor not elsewhere classified (IDH1, IDH2: wild-type; Multiplex Ligation-Dependent Probe Amplification: no BRAF-V600e mutation or BRAF-KIAA1549-fusion or homozygous CDKN2A/B loss, 850 k methylome analysis inconclusive). Postsurgical s-MRI showed no complications (Figure 1F). As it was impossible to resect the entire tumor and the seizure onset zone, it is likely that the patient will not become seizure-free after surgery.</p><p>The case presented illustrates how individualized concepts guide surgical decisions in patients with focal epilepsy due to a tumor in eloquent areas. The aim of removing the most relevant, contrast-enhancing tumor part was achieved without endangering cortical language representations based on solid ESM findings. It was necessary to prioritize avoiding damage to language areas over the complete removal of the tumor and the seizure onset area.</p><p>Robust functional assessment of language representations is critical to minimize the risk of permanent postoperative language deficits. The ESM is the gold standard method for accurately delineating the language-relevant cortex, although the procedure is not yet standardized.<span><sup>2-4</sup></span> As described by Wellmer et al., the type and number of applied language tasks vary between centers.<span><sup>3</sup></span> The l-fMRI allows visualization of hemispheric lateralization of language, but its localization value is not accurate enough to define the margins of surgical resection.<span><sup>4-6</sup></span> For a more rigorous evaluation before and after surgery, NPS assessment of language-associated functions is indispensable.<span><sup>7</sup></span></p><p>The evaluation of functional connectivity in iEEG is promising but has not yet been proven to be as accurate as ESM in iEEG.<span><sup>8</sup></span> Also, awake tumor surgery does not offer similar flexibility in choosing time windows free of afterdischarges and multimodal language tasks for comprehensive language mappings. So, ESM in iEEG remains the gold standard for guiding neurosurgical resection adjacent to cortical language representations.</p>\",\"PeriodicalId\":50508,\"journal\":{\"name\":\"Epileptic Disorders\",\"volume\":\"26 4\",\"pages\":\"548-551\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-05-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/epd2.20245\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Epileptic Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/epd2.20245\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epileptic Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/epd2.20245","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Electrical stimulation mapping guides individualized surgical approach in an epilepsy-associated tumor within language representing cortex
In epilepsy patients with tumors involving the cortex with language representations, a comprehensive interdisciplinary workup is required to protect language function during surgical resection.1
We report the presurgical evaluation of a patient with focal epilepsy due to a progressive tumor in the language area of the left temporal lobe. After non-invasive presurgical diagnostics, we performed an invasive subdural electroencephalogram (iEEG) with extraoperative electrical stimulation mapping (ESM) prior to tumor surgery.2
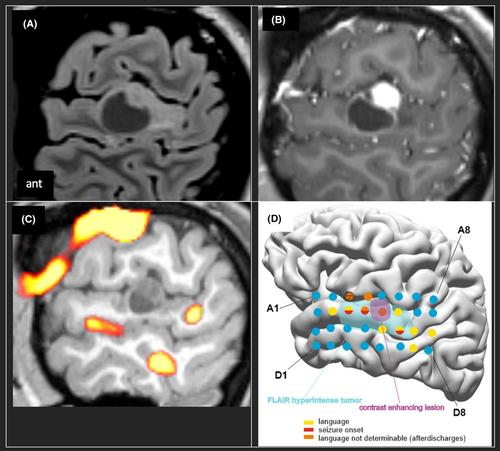
A 22-year-old female university student with left-sided temporal lobe epilepsy was referred for invasive video-EEG monitoring and language mapping to guide resective tumor surgery. Her epilepsy began at the age of 20 years, and it was characterized by focal aware seizures with speech arrest, occasionally followed by focal impaired awareness seizures. Under monotherapy with Levetiracetam up to 4 g/day, she had two to three focal aware seizures/day, despite which she was able to finish her university studies. High-resolution 3T structural magnetic resonance imaging (s-MRI) showed a slowly progressive, partially contrast-enhancing low-grade neuroglial tumor located at the left posterior superior temporal gyrus (Figure 1, Panels A and B) and the basal insula. A functional language MRI (l-fMRI) confirmed left-hemispheric language dominance with activations directly adjacent to the tumor (Figure 1, Panel C). Presurgical neuropsychological assessment (NPS) revealed discrete word-finding difficulties, partly reduced verbal fluency and impaired verbal short-term and working memory performance. The right-handed patient had a normal physical examination. Written informed consent was obtained for the scientific publication of the patient's clinical data.
Invasive video-EEG monitoring for 4 days with a 32-contact subdural grid implanted over the left temporal lobe was performed (Figure 1, Panel D). The ESM language cortical mapping with 50 Hz (biphasic pulses, duration 250 μs, bipolar stimulation up to 15 mA, referential stimulation up to 18 mA) comprised six different language tasks as described in detail before.3 Language representations were identified in contacts B2-3, B6, C5-C8, and D7 (Figure 1, Panel D). The language representation around contacts A3-4 and B4-5 could not be assessed due to unavoidable afterdischarges despite the additional use of lorazepam. In summary, the ESM showed a clear overlap of language representation and tumor in the left superior temporal gyrus. The irritative zone and the seizure onset zone overlapped with language representations (Figure 1, Panel D).
Due to the tumor's location, only the contrast-enhancing solid component and the cyst membrane could be resected via a transsylvian approach to minimize the risk of postoperative language deficits. No need for awake surgery with additional intraoperative language mapping was seen. The postsurgical NPS revealed unchanged performance, especially in language-related tasks, and no deterioration was found. The neuropathological diagnosis was a low-grade neuroepithelial tumor not elsewhere classified (IDH1, IDH2: wild-type; Multiplex Ligation-Dependent Probe Amplification: no BRAF-V600e mutation or BRAF-KIAA1549-fusion or homozygous CDKN2A/B loss, 850 k methylome analysis inconclusive). Postsurgical s-MRI showed no complications (Figure 1F). As it was impossible to resect the entire tumor and the seizure onset zone, it is likely that the patient will not become seizure-free after surgery.
The case presented illustrates how individualized concepts guide surgical decisions in patients with focal epilepsy due to a tumor in eloquent areas. The aim of removing the most relevant, contrast-enhancing tumor part was achieved without endangering cortical language representations based on solid ESM findings. It was necessary to prioritize avoiding damage to language areas over the complete removal of the tumor and the seizure onset area.
Robust functional assessment of language representations is critical to minimize the risk of permanent postoperative language deficits. The ESM is the gold standard method for accurately delineating the language-relevant cortex, although the procedure is not yet standardized.2-4 As described by Wellmer et al., the type and number of applied language tasks vary between centers.3 The l-fMRI allows visualization of hemispheric lateralization of language, but its localization value is not accurate enough to define the margins of surgical resection.4-6 For a more rigorous evaluation before and after surgery, NPS assessment of language-associated functions is indispensable.7
The evaluation of functional connectivity in iEEG is promising but has not yet been proven to be as accurate as ESM in iEEG.8 Also, awake tumor surgery does not offer similar flexibility in choosing time windows free of afterdischarges and multimodal language tasks for comprehensive language mappings. So, ESM in iEEG remains the gold standard for guiding neurosurgical resection adjacent to cortical language representations.
期刊介绍:
Epileptic Disorders is the leading forum where all experts and medical studentswho wish to improve their understanding of epilepsy and related disorders can share practical experiences surrounding diagnosis and care, natural history, and management of seizures.
Epileptic Disorders is the official E-journal of the International League Against Epilepsy for educational communication. As the journal celebrates its 20th anniversary, it will now be available only as an online version. Its mission is to create educational links between epileptologists and other health professionals in clinical practice and scientists or physicians in research-based institutions. This change is accompanied by an increase in the number of issues per year, from 4 to 6, to ensure regular diffusion of recently published material (high quality Review and Seminar in Epileptology papers; Original Research articles or Case reports of educational value; MultiMedia Teaching Material), to serve the global medical community that cares for those affected by epilepsy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


