{"title":"基于模型的 ATG 在 αβhaplo-HSCT 中可促进移植、加快 T 细胞恢复并降低急性 GvHD 的风险。","authors":"","doi":"10.1016/j.jtct.2024.05.015","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>In αβ T-cell/CD19 B-cell depleted hematopoietic stem cell transplantation (αβhaplo-HSCT) recipients, antithymocyte globulin (ATG; Thymoglobulin) is used for preventing graft rejection<span> and graft-versus-host disease (GVHD). The optimal dosing remains to be established, however. Here we present the first comparative analysis of 3 different ATG dosing strategies and their impact on immune reconstitution and </span></span>GVHD. Our study aimed to evaluate the effects of 3 distinct dosing strategies of ATG on engraftment success, αβ</span><sup>+</sup> and γδ<sup>+</sup><span> T cell immune reconstitution, and the incidence and severity of acute GVHD in recipients of αβhaplo-HSCT. This comparative analysis included 3 cohorts of pediatric patients with malignant (n = 36) or nonmalignant (n = 8) disease. Cohorts 1 and 2 were given fixed ATG doses, whereas cohort 3 received doses via a new nomogram, based on absolute lymphocyte count (ALC) and body weight (BW). Cohort 3 showed a 0% incidence of day 100 grade II-IV acute GVHD, compared to 48% in cohort 1 and 27% in cohort 2. Furthermore, cohort 3 (the ALC/BW-based cohort) had a significant increase in CD4</span><sup>+</sup><span> and CD8</span><sup>+</sup> naïve T cells by day 90 (<em>P</em> = .04 and .03, respectively). Additionally, we found that the reconstitution and maturation of γδ<sup>+</sup> T cells post-HSCT was not impacted across all 3 cohorts. Cumulative ATG exposure in all cohorts was lower than previously reported in T cell-replete settings, with a lower pre-HSCT exposure (<40 AU*day/mL) correlating with engraftment failure (<em>P</em> = .007). Conversely, a post-HSCT ATG exposure of 10 to 15 AU*day/mL was optimal for improving day 100 CD4<sup>+</sup> (<em>P</em><span> = .058) and CD8</span><sup>+</sup> (<em>P</em><span> = .03) immune reconstitution without increasing the risk of relapse or nonrelapse mortality. This study represents the first comparative analysis of ATG exposure in αβhaplo-HSCT recipients. Our findings indicate that (1) a 1- to 2-fold ATG to ATLG<span> bioequivalence is more effective than previously established standards, and (2) ATG exposure post-HSCT does not adversely affect γδ</span></span><sup>+</sup> T cell immune reconstitution. Furthermore, a model-based ATG dosing strategy effectively reduces graft rejection and day 100 acute GVHD while also promoting early CD4<sup>+</sup>/CD8<sup>+</sup> immune reconstitution. These insights suggest that further optimization, including more distal administration of higher ATG doses within an ALC/BW-based strategy, will yield even greater improvements in outcomes.</p></div>","PeriodicalId":23283,"journal":{"name":"Transplantation and Cellular Therapy","volume":null,"pages":null},"PeriodicalIF":3.6000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Model-Based Antithymocyte Globulin in αβhaplo-Hematopoietic Stem Cell Transplantation Facilitates Engraftment, Expedites T Cell Recovery, and Mitigates the Risk of Acute Graft-versus-Host Disease\",\"authors\":\"\",\"doi\":\"10.1016/j.jtct.2024.05.015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span>In αβ T-cell/CD19 B-cell depleted hematopoietic stem cell transplantation (αβhaplo-HSCT) recipients, antithymocyte globulin (ATG; Thymoglobulin) is used for preventing graft rejection<span> and graft-versus-host disease (GVHD). The optimal dosing remains to be established, however. Here we present the first comparative analysis of 3 different ATG dosing strategies and their impact on immune reconstitution and </span></span>GVHD. Our study aimed to evaluate the effects of 3 distinct dosing strategies of ATG on engraftment success, αβ</span><sup>+</sup> and γδ<sup>+</sup><span> T cell immune reconstitution, and the incidence and severity of acute GVHD in recipients of αβhaplo-HSCT. This comparative analysis included 3 cohorts of pediatric patients with malignant (n = 36) or nonmalignant (n = 8) disease. Cohorts 1 and 2 were given fixed ATG doses, whereas cohort 3 received doses via a new nomogram, based on absolute lymphocyte count (ALC) and body weight (BW). Cohort 3 showed a 0% incidence of day 100 grade II-IV acute GVHD, compared to 48% in cohort 1 and 27% in cohort 2. Furthermore, cohort 3 (the ALC/BW-based cohort) had a significant increase in CD4</span><sup>+</sup><span> and CD8</span><sup>+</sup> naïve T cells by day 90 (<em>P</em> = .04 and .03, respectively). Additionally, we found that the reconstitution and maturation of γδ<sup>+</sup> T cells post-HSCT was not impacted across all 3 cohorts. Cumulative ATG exposure in all cohorts was lower than previously reported in T cell-replete settings, with a lower pre-HSCT exposure (<40 AU*day/mL) correlating with engraftment failure (<em>P</em> = .007). Conversely, a post-HSCT ATG exposure of 10 to 15 AU*day/mL was optimal for improving day 100 CD4<sup>+</sup> (<em>P</em><span> = .058) and CD8</span><sup>+</sup> (<em>P</em><span> = .03) immune reconstitution without increasing the risk of relapse or nonrelapse mortality. This study represents the first comparative analysis of ATG exposure in αβhaplo-HSCT recipients. Our findings indicate that (1) a 1- to 2-fold ATG to ATLG<span> bioequivalence is more effective than previously established standards, and (2) ATG exposure post-HSCT does not adversely affect γδ</span></span><sup>+</sup> T cell immune reconstitution. Furthermore, a model-based ATG dosing strategy effectively reduces graft rejection and day 100 acute GVHD while also promoting early CD4<sup>+</sup>/CD8<sup>+</sup> immune reconstitution. These insights suggest that further optimization, including more distal administration of higher ATG doses within an ALC/BW-based strategy, will yield even greater improvements in outcomes.</p></div>\",\"PeriodicalId\":23283,\"journal\":{\"name\":\"Transplantation and Cellular Therapy\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation and Cellular Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666636724004123\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation and Cellular Therapy","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666636724004123","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Model-Based Antithymocyte Globulin in αβhaplo-Hematopoietic Stem Cell Transplantation Facilitates Engraftment, Expedites T Cell Recovery, and Mitigates the Risk of Acute Graft-versus-Host Disease
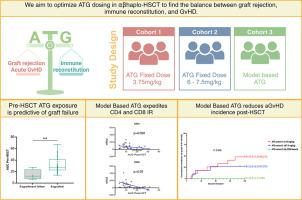
In αβ T-cell/CD19 B-cell depleted hematopoietic stem cell transplantation (αβhaplo-HSCT) recipients, antithymocyte globulin (ATG; Thymoglobulin) is used for preventing graft rejection and graft-versus-host disease (GVHD). The optimal dosing remains to be established, however. Here we present the first comparative analysis of 3 different ATG dosing strategies and their impact on immune reconstitution and GVHD. Our study aimed to evaluate the effects of 3 distinct dosing strategies of ATG on engraftment success, αβ+ and γδ+ T cell immune reconstitution, and the incidence and severity of acute GVHD in recipients of αβhaplo-HSCT. This comparative analysis included 3 cohorts of pediatric patients with malignant (n = 36) or nonmalignant (n = 8) disease. Cohorts 1 and 2 were given fixed ATG doses, whereas cohort 3 received doses via a new nomogram, based on absolute lymphocyte count (ALC) and body weight (BW). Cohort 3 showed a 0% incidence of day 100 grade II-IV acute GVHD, compared to 48% in cohort 1 and 27% in cohort 2. Furthermore, cohort 3 (the ALC/BW-based cohort) had a significant increase in CD4+ and CD8+ naïve T cells by day 90 (P = .04 and .03, respectively). Additionally, we found that the reconstitution and maturation of γδ+ T cells post-HSCT was not impacted across all 3 cohorts. Cumulative ATG exposure in all cohorts was lower than previously reported in T cell-replete settings, with a lower pre-HSCT exposure (<40 AU*day/mL) correlating with engraftment failure (P = .007). Conversely, a post-HSCT ATG exposure of 10 to 15 AU*day/mL was optimal for improving day 100 CD4+ (P = .058) and CD8+ (P = .03) immune reconstitution without increasing the risk of relapse or nonrelapse mortality. This study represents the first comparative analysis of ATG exposure in αβhaplo-HSCT recipients. Our findings indicate that (1) a 1- to 2-fold ATG to ATLG bioequivalence is more effective than previously established standards, and (2) ATG exposure post-HSCT does not adversely affect γδ+ T cell immune reconstitution. Furthermore, a model-based ATG dosing strategy effectively reduces graft rejection and day 100 acute GVHD while also promoting early CD4+/CD8+ immune reconstitution. These insights suggest that further optimization, including more distal administration of higher ATG doses within an ALC/BW-based strategy, will yield even greater improvements in outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


