Hydrosalpinx treatment before in-vitro fertilization: systematic review and network meta-analysis.
Objective: To compare the safety and effectiveness of different methods, both ablative and non-ablative, to treat hydrosalpinx in infertile patients before in-vitro fertilization embryo transfer (IVF-ET) via a systematic review and network meta-analysis (NMA).
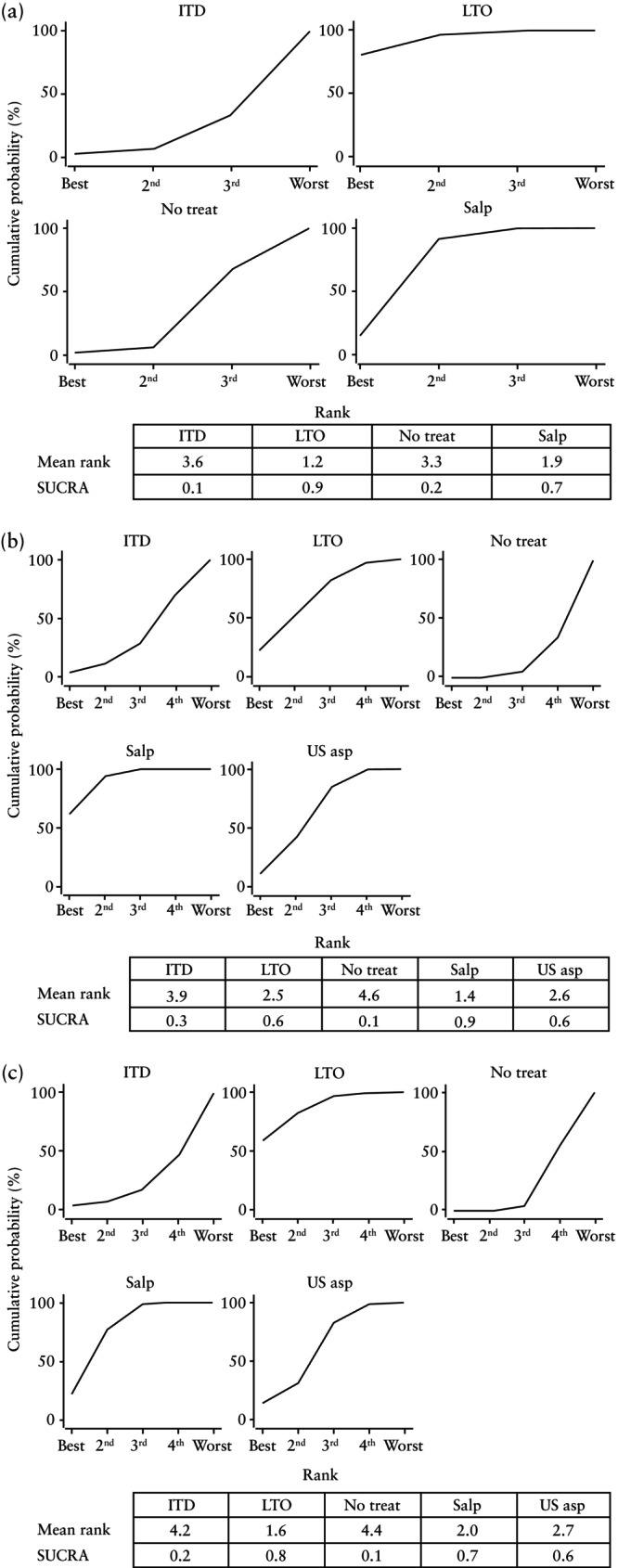
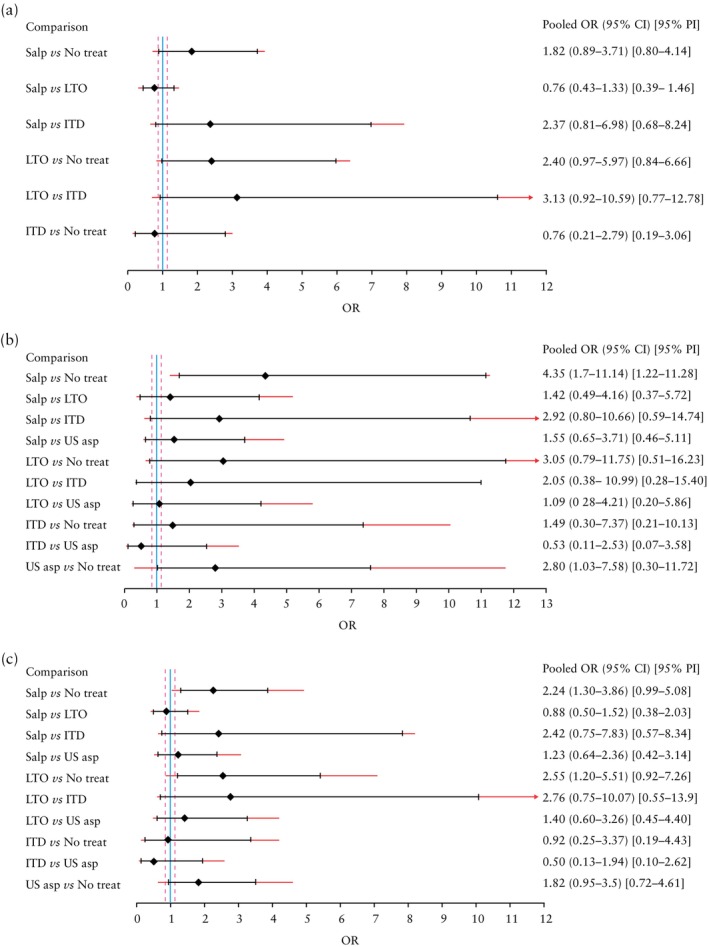
Methods: A structured literature search was conducted in common citation databases. Eligibility criteria included peer-reviewed randomized controlled trials (RCTs) or cohort studies comparing the effectiveness and/or safety of different hydrosalpinx treatments, including salpingectomy, laparoscopic proximal tubal occlusion (LTO), insertion of an intratubal device (ITD), ultrasound-guided aspiration, sclerotherapy and expectant management. Primary outcomes were live birth, ongoing pregnancy and clinical pregnancy. Miscarriage, ectopic pregnancy and procedural complications were considered as secondary outcomes. The main NMA included only RCTs, while observational studies were included in a secondary aggregate NMA. Pooled effects were summarized as odds ratios (ORs) with 95% CI for direct and indirect comparisons, derived from random-effects models. Imprecision of NMA estimates was assessed by comparison of their 95% CIs with predefined thresholds for effect size considered to represent clinical relevance (OR < 0.9 or >1.1). Heterogeneity for NMA findings was estimated using the variance of the distribution of the underlying treatment effects (τ2), expressed as a 95% prediction interval. Surface under the cumulative ranking curve (SUCRA) was used to predict relative treatment rankings for each outcome.
Results: The main analysis included nine RCTs, while an additional 17 observational studies were incorporated into the aggregate analysis. The NMA of RCTs revealed no significant differences in live birth rate between hydrosalpinx treatment methods, with LTO achieving the highest SUCRA value (0.9). Salpingectomy and ultrasound-guided aspiration significantly increased the ongoing pregnancy rate compared with no treatment (OR, 4.35 (95% CI, 1.70-11.14) and 2.80 (95% CI, 1.03-7.58), respectively), with salpingectomy having the highest SUCRA value (0.9). Clinical pregnancy rate was significantly higher following salpingectomy (OR, 2.24 (95% CI, 1.30-3.86)) and LTO (OR, 2.55 (95% CI, 1.20-5.51)) compared with no treatment, despite some heterogeneity; LTO had the highest SUCRA value (0.8). NMA showed no significant differences in secondary outcomes between treatments. Aggregate NMA indicated that sclerotherapy significantly increased the live birth rate compared with no treatment. Higher ongoing pregnancy rate was observed in patients treated with salpingectomy, ultrasound-guided aspiration and LTO compared to untreated patients, with salpingectomy having the highest SUCRA value (0.9). Except for ITD insertion, all interventions increased the clinical pregnancy rate compared with no treatment. LTO had a greater effect on clinical pregnancy rate compared to ultrasound-guided aspiration, with no significant differences in other pairwise comparisons. NMA ranked LTO as the most effective treatment for increasing the clinical pregnancy rate and reducing the miscarriage rate, while sclerotherapy was deemed safer with regard to the ovarian response to IVF stimulation.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


