{"title":"膀胱切除术后输尿管狭窄:侧特异性风险因素和放射学评估","authors":"Simone Buchardt Brandt, Lotte Ibsen, Gitte Wrist Lam, Morten Bøttcher, Pernille Skjold Kingo, Jørgen Bjerggaard Jensen","doi":"10.1002/bco2.364","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>To evaluate risk factors contributing to side-specific benign ureteroenteric strictures following radical cystectomy with an ileal conduit.</p>\n </section>\n \n <section>\n \n <h3> Materials and Methods</h3>\n \n <p>Data obtained from patients with bladder cancer who underwent radical cystectomy with ileal conduit surgery between 2015 and 2018 were retrospectively analysed. Imaging prior to surgery was analysed, regarding calcifications in the aorta, sarcopenia and postoperatively for length of remaining left ureter. Descriptive analyses were performed on preoperative and perioperative data, comparing patients who developed unilateral left- or right-sided strictures, bilateral strictures, to those who remained free of strictures. COX regression analysis was employed to calculate crude and adjusted hazard ratio for side-specific strictures.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The study included 395 patients. Strictures developed in 19% (75/395) of the patients, within a median period of 9 months: 57% (43/75) unilateral left sided, 20% (15/75) unilateral right sided and 23% (17/75) bilateral. Unilateral left-sided stricture was associated with higher body mass index (<i>p</i> = 0.077) and hypercholesterolemia (<i>p</i> = 0.007). Right-sided stricture was associated with a history of prior abdominal surgery (<i>p</i> = 0.029) and postoperative leakage (<i>p</i> = 0.004). Bilateral stricture was associated with smoking (<i>p</i> = 0.006) and high BMI (<i>p</i> = 0.015). The adjusted HR comparing patients with and without previous abdominal surgery was only significantly higher for right-sided ureteroenteric strictures (HR 3.18 [95% CI: 1.11; 9.05]) compared with patients without strictures. No association was identified between strictures and preoperative aortic calcification of the abdominal aorta or sarcopenia as estimated from imaging.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The aetiology of ureteroenteric strictures appears multifactorial. Our findings suggest that development of left-sided stricture is influenced by factors associated with metabolic syndrome, indicating a potential role of distal ureteric ischemia. On the other hand, right-sided stricture was more frequent in patients with previous abdominal surgery and postoperative leakage.</p>\n </section>\n </div>","PeriodicalId":72420,"journal":{"name":"BJUI compass","volume":"5 7","pages":"699-708"},"PeriodicalIF":1.6000,"publicationDate":"2024-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/bco2.364","citationCount":"0","resultStr":"{\"title\":\"Ureteroenteric strictures after cystectomy: Side-specific risk factors and radiological assessment\",\"authors\":\"Simone Buchardt Brandt, Lotte Ibsen, Gitte Wrist Lam, Morten Bøttcher, Pernille Skjold Kingo, Jørgen Bjerggaard Jensen\",\"doi\":\"10.1002/bco2.364\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>To evaluate risk factors contributing to side-specific benign ureteroenteric strictures following radical cystectomy with an ileal conduit.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Materials and Methods</h3>\\n \\n <p>Data obtained from patients with bladder cancer who underwent radical cystectomy with ileal conduit surgery between 2015 and 2018 were retrospectively analysed. Imaging prior to surgery was analysed, regarding calcifications in the aorta, sarcopenia and postoperatively for length of remaining left ureter. Descriptive analyses were performed on preoperative and perioperative data, comparing patients who developed unilateral left- or right-sided strictures, bilateral strictures, to those who remained free of strictures. COX regression analysis was employed to calculate crude and adjusted hazard ratio for side-specific strictures.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The study included 395 patients. Strictures developed in 19% (75/395) of the patients, within a median period of 9 months: 57% (43/75) unilateral left sided, 20% (15/75) unilateral right sided and 23% (17/75) bilateral. Unilateral left-sided stricture was associated with higher body mass index (<i>p</i> = 0.077) and hypercholesterolemia (<i>p</i> = 0.007). Right-sided stricture was associated with a history of prior abdominal surgery (<i>p</i> = 0.029) and postoperative leakage (<i>p</i> = 0.004). Bilateral stricture was associated with smoking (<i>p</i> = 0.006) and high BMI (<i>p</i> = 0.015). The adjusted HR comparing patients with and without previous abdominal surgery was only significantly higher for right-sided ureteroenteric strictures (HR 3.18 [95% CI: 1.11; 9.05]) compared with patients without strictures. No association was identified between strictures and preoperative aortic calcification of the abdominal aorta or sarcopenia as estimated from imaging.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>The aetiology of ureteroenteric strictures appears multifactorial. Our findings suggest that development of left-sided stricture is influenced by factors associated with metabolic syndrome, indicating a potential role of distal ureteric ischemia. On the other hand, right-sided stricture was more frequent in patients with previous abdominal surgery and postoperative leakage.</p>\\n </section>\\n </div>\",\"PeriodicalId\":72420,\"journal\":{\"name\":\"BJUI compass\",\"volume\":\"5 7\",\"pages\":\"699-708\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/bco2.364\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJUI compass\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/bco2.364\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJUI compass","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/bco2.364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Ureteroenteric strictures after cystectomy: Side-specific risk factors and radiological assessment
Objective
To evaluate risk factors contributing to side-specific benign ureteroenteric strictures following radical cystectomy with an ileal conduit.
Materials and Methods
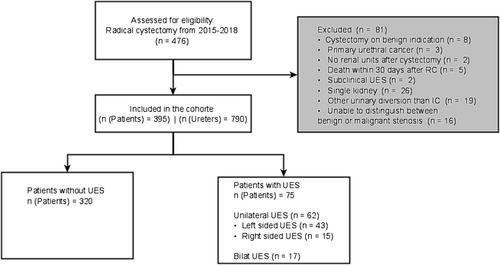
Data obtained from patients with bladder cancer who underwent radical cystectomy with ileal conduit surgery between 2015 and 2018 were retrospectively analysed. Imaging prior to surgery was analysed, regarding calcifications in the aorta, sarcopenia and postoperatively for length of remaining left ureter. Descriptive analyses were performed on preoperative and perioperative data, comparing patients who developed unilateral left- or right-sided strictures, bilateral strictures, to those who remained free of strictures. COX regression analysis was employed to calculate crude and adjusted hazard ratio for side-specific strictures.
Results
The study included 395 patients. Strictures developed in 19% (75/395) of the patients, within a median period of 9 months: 57% (43/75) unilateral left sided, 20% (15/75) unilateral right sided and 23% (17/75) bilateral. Unilateral left-sided stricture was associated with higher body mass index (p = 0.077) and hypercholesterolemia (p = 0.007). Right-sided stricture was associated with a history of prior abdominal surgery (p = 0.029) and postoperative leakage (p = 0.004). Bilateral stricture was associated with smoking (p = 0.006) and high BMI (p = 0.015). The adjusted HR comparing patients with and without previous abdominal surgery was only significantly higher for right-sided ureteroenteric strictures (HR 3.18 [95% CI: 1.11; 9.05]) compared with patients without strictures. No association was identified between strictures and preoperative aortic calcification of the abdominal aorta or sarcopenia as estimated from imaging.
Conclusion
The aetiology of ureteroenteric strictures appears multifactorial. Our findings suggest that development of left-sided stricture is influenced by factors associated with metabolic syndrome, indicating a potential role of distal ureteric ischemia. On the other hand, right-sided stricture was more frequent in patients with previous abdominal surgery and postoperative leakage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


