Parvathy Krishnan, Nilima Jawale, Adam Sodikoff, Susan R Malfa, Kathleen McCarthy, Lisa M Strickrodt, Diana D'Agrosa, Alexandra Pickard, Lance A Parton, Meenakshi Singh
{"title":"协同安全:在新生儿重症监护室通过共同决策减少意外拔管的定制方法。","authors":"Parvathy Krishnan, Nilima Jawale, Adam Sodikoff, Susan R Malfa, Kathleen McCarthy, Lisa M Strickrodt, Diana D'Agrosa, Alexandra Pickard, Lance A Parton, Meenakshi Singh","doi":"10.1097/pq9.0000000000000729","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unplanned Extubation (UE) remains an important patient safety issue in the Neonatal Intensive Care Unit. Our SMART AIM was to decrease the rate of UE by 10% from the baseline from January to December 2022 by emphasizing collaboration among healthcare professionals and through the use of shared decision-making.</p><p><strong>Methods: </strong>We established an interdisciplinary Quality Improvement team composed of nurses, respiratory therapists, and physicians (MDs). The definition of UE was standardized. UE was audited using an apparent cause analysis form to discern associated causes and pinpoint areas for improvement. Interventions were implemented in a step-by-step fashion and reviewed monthly using the model for improvement. A shared decision-making approach fostered collaborative problem-solving.</p><p><strong>Results: </strong>Our baseline UE rate was 2.3 per 100 ventilator days. Retaping, general bedside care, and position change accounted for over 50% of the UE events in 2022. The rate of UE was reduced by 48% by the end of December 2022. We achieved special-cause variation by the end of March 2023.</p><p><strong>Conclusions: </strong>The sole education of medical and nursing providers about various approaches to decreasing unnecessary retaping was ineffective in reducing UE rates. Shared decision-making incorporating inputs from nurses, respiratory therapists, and MDs led to a substantial reduction in the UE rate and underscores the potential of systematic evaluation of risk factors combined with collaborative best practices.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e729"},"PeriodicalIF":1.1000,"publicationDate":"2024-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11093562/pdf/","citationCount":"0","resultStr":"{\"title\":\"Synergizing Safety: A Customized Approach to Curtailing Unplanned Extubations through Shared Decision-making in the NICU.\",\"authors\":\"Parvathy Krishnan, Nilima Jawale, Adam Sodikoff, Susan R Malfa, Kathleen McCarthy, Lisa M Strickrodt, Diana D'Agrosa, Alexandra Pickard, Lance A Parton, Meenakshi Singh\",\"doi\":\"10.1097/pq9.0000000000000729\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Unplanned Extubation (UE) remains an important patient safety issue in the Neonatal Intensive Care Unit. Our SMART AIM was to decrease the rate of UE by 10% from the baseline from January to December 2022 by emphasizing collaboration among healthcare professionals and through the use of shared decision-making.</p><p><strong>Methods: </strong>We established an interdisciplinary Quality Improvement team composed of nurses, respiratory therapists, and physicians (MDs). The definition of UE was standardized. UE was audited using an apparent cause analysis form to discern associated causes and pinpoint areas for improvement. Interventions were implemented in a step-by-step fashion and reviewed monthly using the model for improvement. A shared decision-making approach fostered collaborative problem-solving.</p><p><strong>Results: </strong>Our baseline UE rate was 2.3 per 100 ventilator days. Retaping, general bedside care, and position change accounted for over 50% of the UE events in 2022. The rate of UE was reduced by 48% by the end of December 2022. We achieved special-cause variation by the end of March 2023.</p><p><strong>Conclusions: </strong>The sole education of medical and nursing providers about various approaches to decreasing unnecessary retaping was ineffective in reducing UE rates. Shared decision-making incorporating inputs from nurses, respiratory therapists, and MDs led to a substantial reduction in the UE rate and underscores the potential of systematic evaluation of risk factors combined with collaborative best practices.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"9 3\",\"pages\":\"e729\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-05-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11093562/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000729\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000729","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Synergizing Safety: A Customized Approach to Curtailing Unplanned Extubations through Shared Decision-making in the NICU.
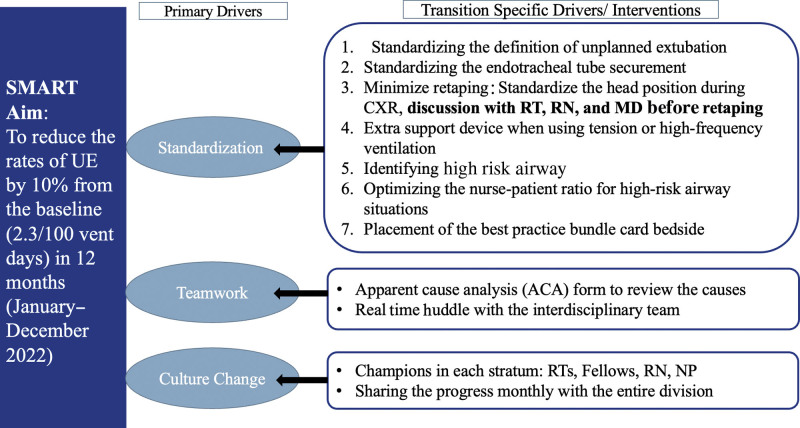
Background: Unplanned Extubation (UE) remains an important patient safety issue in the Neonatal Intensive Care Unit. Our SMART AIM was to decrease the rate of UE by 10% from the baseline from January to December 2022 by emphasizing collaboration among healthcare professionals and through the use of shared decision-making.
Methods: We established an interdisciplinary Quality Improvement team composed of nurses, respiratory therapists, and physicians (MDs). The definition of UE was standardized. UE was audited using an apparent cause analysis form to discern associated causes and pinpoint areas for improvement. Interventions were implemented in a step-by-step fashion and reviewed monthly using the model for improvement. A shared decision-making approach fostered collaborative problem-solving.
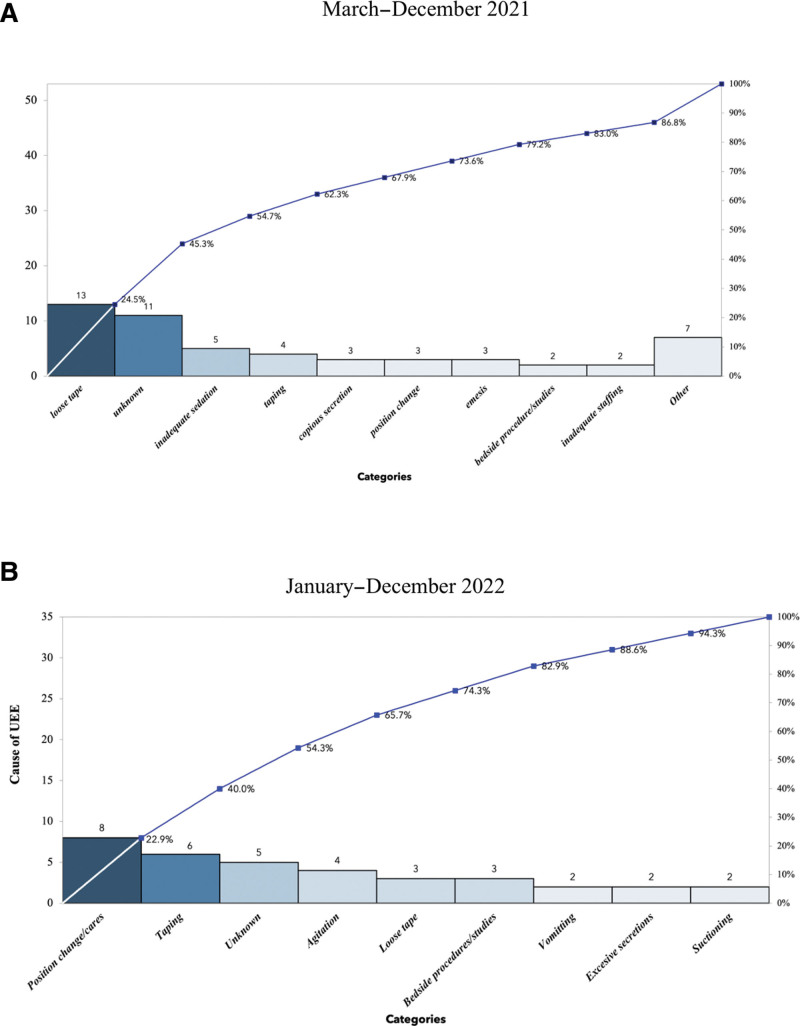
Results: Our baseline UE rate was 2.3 per 100 ventilator days. Retaping, general bedside care, and position change accounted for over 50% of the UE events in 2022. The rate of UE was reduced by 48% by the end of December 2022. We achieved special-cause variation by the end of March 2023.
Conclusions: The sole education of medical and nursing providers about various approaches to decreasing unnecessary retaping was ineffective in reducing UE rates. Shared decision-making incorporating inputs from nurses, respiratory therapists, and MDs led to a substantial reduction in the UE rate and underscores the potential of systematic evaluation of risk factors combined with collaborative best practices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


