Julia G Harris, Jordan T Jones, Leslie Favier, Emily Fox, Michael J Holland, Amy Ivy, Cara M Hoffart, Maria Ibarra, Ashley M Cooper
{"title":"提高免疫抑制性风湿病儿科患者的肺炎球菌疫苗接种率。","authors":"Julia G Harris, Jordan T Jones, Leslie Favier, Emily Fox, Michael J Holland, Amy Ivy, Cara M Hoffart, Maria Ibarra, Ashley M Cooper","doi":"10.1097/pq9.0000000000000725","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with rheumatic diseases are at a high risk of invasive pneumococcal disease due to immunosuppression. We conducted a quality improvement project, and the first aim was to increase the percentage of patients with systemic lupus erythematosus and mixed connective tissue disease that is up to date on pneumococcal vaccinations from 9.6% to 80% within one year. Subsequently, the second aim was to increase the percentage of patients on immunosuppression with systemic lupus erythematosus, mixed connective tissue disease, juvenile dermatomyositis and systemic vasculitis that is up to date on pneumococcal vaccinations from 62.6% to 80% within one year.</p><p><strong>Methods: </strong>Two process measures were up-to-date vaccination status on (1) 13-valent pneumococcal conjugated vaccine (PCV13) and (2) 23-valent pneumococcal polysaccharide vaccine (PPSV23). Our outcome measure was being fully up to date on both pneumococcal vaccinations. Interventions included an immunization algorithm, reporting of eligible patients, education, reminders, and pre-visit planning.</p><p><strong>Results: </strong>There were shifts in the centerline for all quality measures in both phases of this project. The combined pneumococcal vaccination rate for Phase 1 increased from 9.6% to 91.1%, and this centerline was sustained. Pneumococcal vaccination rates also significantly increased for Phase 2: 68.8% to 93.4% for PCV13, 65.2% to 88.5% for PPSV23, and 62.6% to 86.5% for the combined pneumococcal vaccination rate.</p><p><strong>Conclusions: </strong>Quality improvement methodology significantly increased and sustained pneumococcal vaccination rates in our high-risk, immunosuppressed patients. We continue to prioritize this important initiative to mitigate the risk of invasive pneumococcal disease.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e725"},"PeriodicalIF":1.1000,"publicationDate":"2024-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11093563/pdf/","citationCount":"0","resultStr":"{\"title\":\"Improving Pneumococcal Vaccination Rates in Immunosuppressed Pediatric Patients with Rheumatic Disease.\",\"authors\":\"Julia G Harris, Jordan T Jones, Leslie Favier, Emily Fox, Michael J Holland, Amy Ivy, Cara M Hoffart, Maria Ibarra, Ashley M Cooper\",\"doi\":\"10.1097/pq9.0000000000000725\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with rheumatic diseases are at a high risk of invasive pneumococcal disease due to immunosuppression. We conducted a quality improvement project, and the first aim was to increase the percentage of patients with systemic lupus erythematosus and mixed connective tissue disease that is up to date on pneumococcal vaccinations from 9.6% to 80% within one year. Subsequently, the second aim was to increase the percentage of patients on immunosuppression with systemic lupus erythematosus, mixed connective tissue disease, juvenile dermatomyositis and systemic vasculitis that is up to date on pneumococcal vaccinations from 62.6% to 80% within one year.</p><p><strong>Methods: </strong>Two process measures were up-to-date vaccination status on (1) 13-valent pneumococcal conjugated vaccine (PCV13) and (2) 23-valent pneumococcal polysaccharide vaccine (PPSV23). Our outcome measure was being fully up to date on both pneumococcal vaccinations. Interventions included an immunization algorithm, reporting of eligible patients, education, reminders, and pre-visit planning.</p><p><strong>Results: </strong>There were shifts in the centerline for all quality measures in both phases of this project. The combined pneumococcal vaccination rate for Phase 1 increased from 9.6% to 91.1%, and this centerline was sustained. Pneumococcal vaccination rates also significantly increased for Phase 2: 68.8% to 93.4% for PCV13, 65.2% to 88.5% for PPSV23, and 62.6% to 86.5% for the combined pneumococcal vaccination rate.</p><p><strong>Conclusions: </strong>Quality improvement methodology significantly increased and sustained pneumococcal vaccination rates in our high-risk, immunosuppressed patients. We continue to prioritize this important initiative to mitigate the risk of invasive pneumococcal disease.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"9 3\",\"pages\":\"e725\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-05-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11093563/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000725\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000725","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Improving Pneumococcal Vaccination Rates in Immunosuppressed Pediatric Patients with Rheumatic Disease.
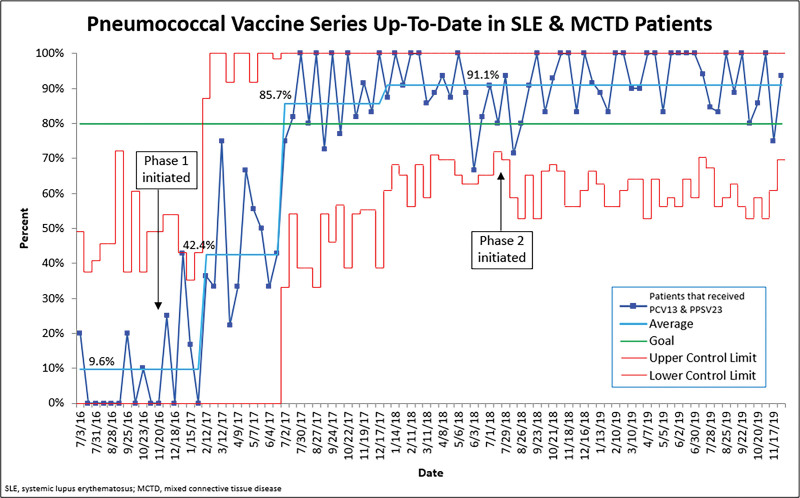
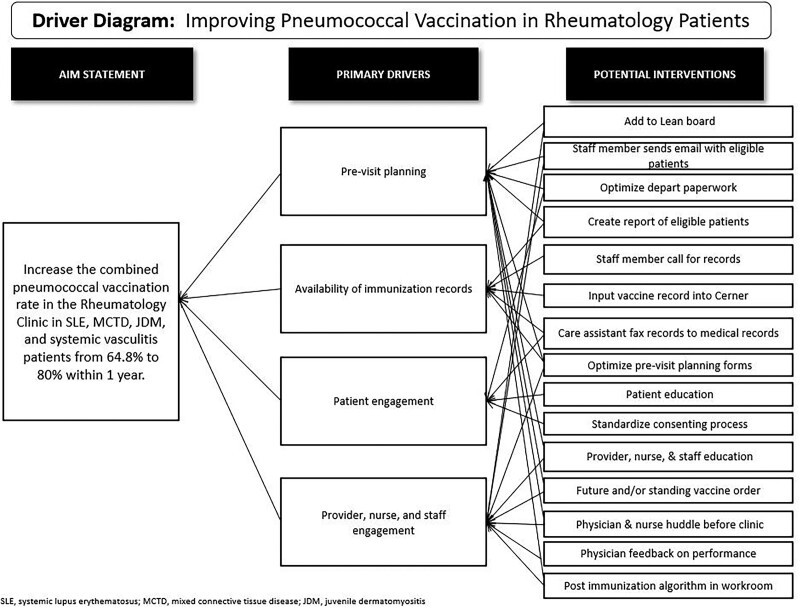
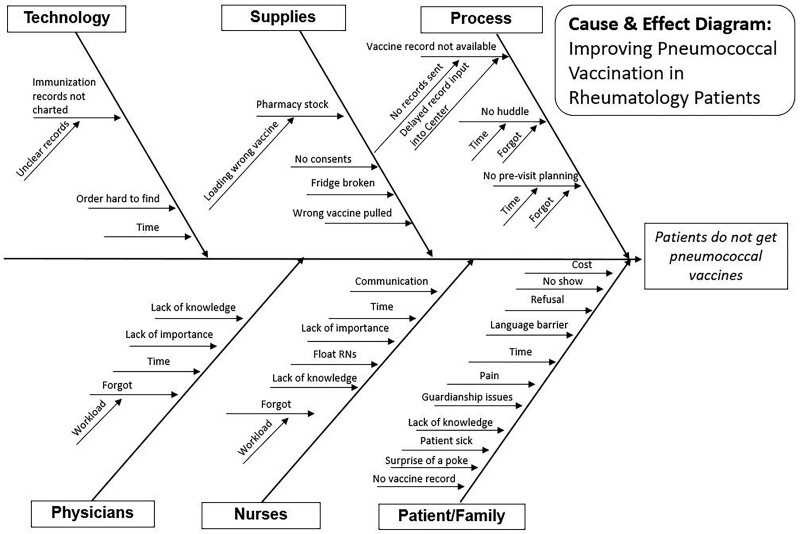
Background: Patients with rheumatic diseases are at a high risk of invasive pneumococcal disease due to immunosuppression. We conducted a quality improvement project, and the first aim was to increase the percentage of patients with systemic lupus erythematosus and mixed connective tissue disease that is up to date on pneumococcal vaccinations from 9.6% to 80% within one year. Subsequently, the second aim was to increase the percentage of patients on immunosuppression with systemic lupus erythematosus, mixed connective tissue disease, juvenile dermatomyositis and systemic vasculitis that is up to date on pneumococcal vaccinations from 62.6% to 80% within one year.
Methods: Two process measures were up-to-date vaccination status on (1) 13-valent pneumococcal conjugated vaccine (PCV13) and (2) 23-valent pneumococcal polysaccharide vaccine (PPSV23). Our outcome measure was being fully up to date on both pneumococcal vaccinations. Interventions included an immunization algorithm, reporting of eligible patients, education, reminders, and pre-visit planning.
Results: There were shifts in the centerline for all quality measures in both phases of this project. The combined pneumococcal vaccination rate for Phase 1 increased from 9.6% to 91.1%, and this centerline was sustained. Pneumococcal vaccination rates also significantly increased for Phase 2: 68.8% to 93.4% for PCV13, 65.2% to 88.5% for PPSV23, and 62.6% to 86.5% for the combined pneumococcal vaccination rate.
Conclusions: Quality improvement methodology significantly increased and sustained pneumococcal vaccination rates in our high-risk, immunosuppressed patients. We continue to prioritize this important initiative to mitigate the risk of invasive pneumococcal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


