Jennifer Lees, Jamie Crowther, Peter Hanlon, Elaine W Butterly, Sarah H Wild, Frances Mair, Bruce Guthrie, Katie Gillies, Sofia Dias, Nicky J Welton, Srinivasa Vittal Katikireddi, David A McAllister
{"title":"慢性病 3/4 期行业资助试验的参与者特征和排除情况:对参与者个人水平数据的荟萃分析。","authors":"Jennifer Lees, Jamie Crowther, Peter Hanlon, Elaine W Butterly, Sarah H Wild, Frances Mair, Bruce Guthrie, Katie Gillies, Sofia Dias, Nicky J Welton, Srinivasa Vittal Katikireddi, David A McAllister","doi":"10.1136/bmjmed-2023-000732","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess whether age, sex, comorbidity count, and race and ethnic group are associated with the likelihood of trial participants not being enrolled in a trial for any reason (ie, screen failure).</p><p><strong>Design: </strong>Bayesian meta-analysis of individual participant level data.</p><p><strong>Setting: </strong>Industry funded phase 3/4 trials of chronic medical conditions.</p><p><strong>Participants: </strong>Participants were identified using individual participant level data to be in either the enrolled group or screen failure group. Data were available for 52 trials involving 72 178 screened individuals of whom 24 733 (34%) were excluded from the trial at the screening stage.</p><p><strong>Main outcome measures: </strong>For each trial, logistic regression models were constructed to assess likelihood of screen failure in people who had been invited to screening, and were regressed on age (per 10 year increment), sex (male <i>v</i> female), comorbidity count (per one additional comorbidity), and race or ethnic group. Trial level analyses were combined in Bayesian hierarchical models with pooling across condition.</p><p><strong>Results: </strong>In age and sex adjusted models across all trials, neither age nor sex was associated with increased odds of screen failure, although weak associations were detected after additionally adjusting for comorbidity (odds ratio of age, per 10 year increment was 1.02 (95% credibility interval 1.01 to 1.04) and male sex (0.95 (0.91 to 1.00)). Comorbidity count was weakly associated with screen failure, but in an unexpected direction (0.97 per additional comorbidity (0.94 to 1.00), adjusted for age and sex). People who self-reported as black seemed to be slightly more likely to fail screening than people reporting as white (1.04 (0.99 to 1.09)); a weak effect that seemed to persist after adjustment for age, sex, and comorbidity count (1.05 (0.98 to 1.12)). The between-trial heterogeneity was generally low, evidence of heterogeneity by sex was noted across conditions (variation in odds ratios on log scale of 0.01-0.13).</p><p><strong>Conclusions: </strong>Although the conclusions are limited by uncertainty about the completeness or accuracy of data collection among participants who were not randomised, we identified mostly weak associations with an increased likelihood of screen failure for age, sex, comorbidity count, and black race or ethnic group. Proportionate increases in screening these underserved populations may improve representation in trials.</p><p><strong>Trial registration number: </strong>PROSPERO CRD42018048202.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"3 1","pages":"e000732"},"PeriodicalIF":10.0000,"publicationDate":"2024-05-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11085787/pdf/","citationCount":"0","resultStr":"{\"title\":\"Participant characteristics and exclusion from phase 3/4 industry funded trials of chronic medical conditions: meta-analysis of individual participant level data.\",\"authors\":\"Jennifer Lees, Jamie Crowther, Peter Hanlon, Elaine W Butterly, Sarah H Wild, Frances Mair, Bruce Guthrie, Katie Gillies, Sofia Dias, Nicky J Welton, Srinivasa Vittal Katikireddi, David A McAllister\",\"doi\":\"10.1136/bmjmed-2023-000732\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To assess whether age, sex, comorbidity count, and race and ethnic group are associated with the likelihood of trial participants not being enrolled in a trial for any reason (ie, screen failure).</p><p><strong>Design: </strong>Bayesian meta-analysis of individual participant level data.</p><p><strong>Setting: </strong>Industry funded phase 3/4 trials of chronic medical conditions.</p><p><strong>Participants: </strong>Participants were identified using individual participant level data to be in either the enrolled group or screen failure group. Data were available for 52 trials involving 72 178 screened individuals of whom 24 733 (34%) were excluded from the trial at the screening stage.</p><p><strong>Main outcome measures: </strong>For each trial, logistic regression models were constructed to assess likelihood of screen failure in people who had been invited to screening, and were regressed on age (per 10 year increment), sex (male <i>v</i> female), comorbidity count (per one additional comorbidity), and race or ethnic group. Trial level analyses were combined in Bayesian hierarchical models with pooling across condition.</p><p><strong>Results: </strong>In age and sex adjusted models across all trials, neither age nor sex was associated with increased odds of screen failure, although weak associations were detected after additionally adjusting for comorbidity (odds ratio of age, per 10 year increment was 1.02 (95% credibility interval 1.01 to 1.04) and male sex (0.95 (0.91 to 1.00)). Comorbidity count was weakly associated with screen failure, but in an unexpected direction (0.97 per additional comorbidity (0.94 to 1.00), adjusted for age and sex). People who self-reported as black seemed to be slightly more likely to fail screening than people reporting as white (1.04 (0.99 to 1.09)); a weak effect that seemed to persist after adjustment for age, sex, and comorbidity count (1.05 (0.98 to 1.12)). The between-trial heterogeneity was generally low, evidence of heterogeneity by sex was noted across conditions (variation in odds ratios on log scale of 0.01-0.13).</p><p><strong>Conclusions: </strong>Although the conclusions are limited by uncertainty about the completeness or accuracy of data collection among participants who were not randomised, we identified mostly weak associations with an increased likelihood of screen failure for age, sex, comorbidity count, and black race or ethnic group. Proportionate increases in screening these underserved populations may improve representation in trials.</p><p><strong>Trial registration number: </strong>PROSPERO CRD42018048202.</p>\",\"PeriodicalId\":72433,\"journal\":{\"name\":\"BMJ medicine\",\"volume\":\"3 1\",\"pages\":\"e000732\"},\"PeriodicalIF\":10.0000,\"publicationDate\":\"2024-05-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11085787/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjmed-2023-000732\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2023-000732","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Participant characteristics and exclusion from phase 3/4 industry funded trials of chronic medical conditions: meta-analysis of individual participant level data.
Objectives: To assess whether age, sex, comorbidity count, and race and ethnic group are associated with the likelihood of trial participants not being enrolled in a trial for any reason (ie, screen failure).
Design: Bayesian meta-analysis of individual participant level data.
Setting: Industry funded phase 3/4 trials of chronic medical conditions.
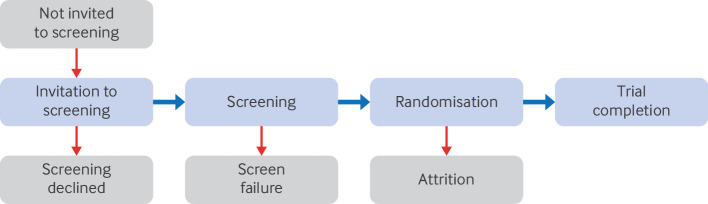
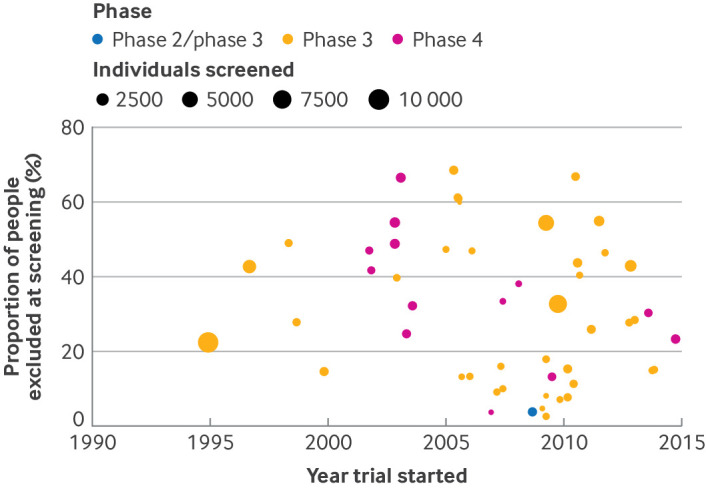
Participants: Participants were identified using individual participant level data to be in either the enrolled group or screen failure group. Data were available for 52 trials involving 72 178 screened individuals of whom 24 733 (34%) were excluded from the trial at the screening stage.
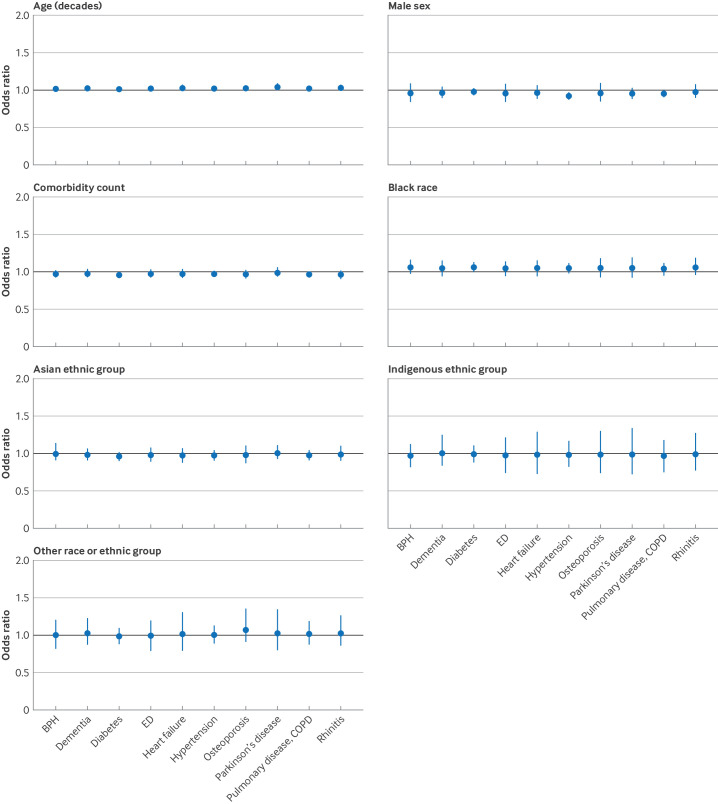
Main outcome measures: For each trial, logistic regression models were constructed to assess likelihood of screen failure in people who had been invited to screening, and were regressed on age (per 10 year increment), sex (male v female), comorbidity count (per one additional comorbidity), and race or ethnic group. Trial level analyses were combined in Bayesian hierarchical models with pooling across condition.
Results: In age and sex adjusted models across all trials, neither age nor sex was associated with increased odds of screen failure, although weak associations were detected after additionally adjusting for comorbidity (odds ratio of age, per 10 year increment was 1.02 (95% credibility interval 1.01 to 1.04) and male sex (0.95 (0.91 to 1.00)). Comorbidity count was weakly associated with screen failure, but in an unexpected direction (0.97 per additional comorbidity (0.94 to 1.00), adjusted for age and sex). People who self-reported as black seemed to be slightly more likely to fail screening than people reporting as white (1.04 (0.99 to 1.09)); a weak effect that seemed to persist after adjustment for age, sex, and comorbidity count (1.05 (0.98 to 1.12)). The between-trial heterogeneity was generally low, evidence of heterogeneity by sex was noted across conditions (variation in odds ratios on log scale of 0.01-0.13).
Conclusions: Although the conclusions are limited by uncertainty about the completeness or accuracy of data collection among participants who were not randomised, we identified mostly weak associations with an increased likelihood of screen failure for age, sex, comorbidity count, and black race or ethnic group. Proportionate increases in screening these underserved populations may improve representation in trials.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


