经主动脉途径进行室间隔中段和室间隔顶部切除术的有效性和安全性
IF 4.9
1区 医学
Q1 CARDIAC & CARDIOVASCULAR SYSTEMS
Journal of Thoracic and Cardiovascular Surgery
Pub Date : 2024-12-01
DOI:10.1016/j.jtcvs.2024.04.016
引用次数: 0
摘要
目的评估肥厚型心肌病伴左心室流出道和/或中室壁阻塞的患者接受经主动脉中室壁和心尖部室间隔肌瘤切除术的安全性和有效性:从2018年1月1日至2023年8月8日,克利夫兰诊所共对940名患者进行了经主动脉室间隔肌瘤切除术,其中682人(73%)进行了室间隔中段和/或心尖部切除术。接受孤立的基底室间隔切除术的患者不包括在内。模板化的手术报告将切除的室间隔区域指定为基底(二尖瓣对侧至瓣叶尖)、中室(瓣叶尖至乳头肌头外)和心尖(心室顶端三分之一处)。对心肌切除标本重量、心室内梯度和临床结果进行了评估:结果:在 682 例患者中,582 例(85%)进行了基底加中室切除,78 例(11%)进行了基底、中室和心尖切除。术前脑室内梯度平均为 102±41 mmHg。切除重量中位数为 10 克(第 15、85 百分位数:7、15),术后室内梯度平均值为 16±10 mmHg,其中 625 例(96%)患者的梯度≤36 mmHg。没有二尖瓣或主动脉瓣的先天性损伤。38例(5.6%)患者需要安置永久起搏器,其中8例(1.2%)术前传导正常。1例(0.1%)患者因术中出现室间隔缺损而死亡:结论:为缓解梗阻而接受室间隔黏膜切除术的大多数患者都需要切除基底室间隔以外的部分。有了专门的器械、详细的成像和对可变室间隔解剖的了解,就可以通过经主动脉方法安全有效地切除室间隔中段和心尖部肌肉。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Efficacy and safety of a transaortic approach to midventricular and apical septal myectomy
Objective
The study objective was to evaluate the safety and efficacy of a transaortic approach to midventricular and apical septal myectomy in patients with hypertrophic cardiomyopathy with left ventricular outflow tract or midventricular obstruction.
Methods
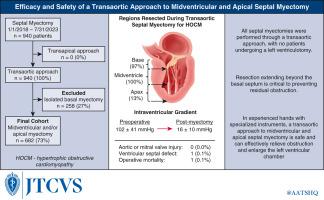
From January 2018 to August 2023, 940 patients underwent transaortic septal myectomy at the Cleveland Clinic, of whom 682 (73%) had midventricular or apical resection. Patients who underwent isolated basal myectomies were excluded. Templated operative reports designated septal regions resected as basal (opposition to mitral valve up to the leaflet tips), midventricular (leaflet tips to just beyond the papillary muscle heads), and apical (apical third of the ventricle). Myocardial resection specimen weights, intraventricular gradients, and clinical outcomes were assessed.
Results
Of the 682 patients, 582 (85%) had basal plus midventricular resection and 78 (11%) had basal, midventricular, and apical resection. Mean preoperative intraventricular gradient was 102 ± 41 mm Hg. Median resection weight was 10 g (15th, 85th percentiles: 7, 15), and mean postoperative intraventricular gradient was 16 ± 10 mm Hg, with 625 (96%) patients achieving gradients 36 mm Hg or less. There were no iatrogenic mitral or aortic valve injuries. Permanent pacemaker placement was required in 38 patients (5.6%), of whom 8 (1.2%) had normal preoperative conduction. Operative mortality occurred in 1 patient (0.1%) after an intraoperative ventricular septal defect.
Conclusions
Most patients undergoing septal myectomy for relief of obstruction required resection beyond the basal septum. With specialized instrumentation, detailed imaging and knowledge of variable septal anatomy, resecting midventricular and apical septal muscle can be safely and effectively achieved through a transaortic approach.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

CiteScore
11.20
自引率
10.00%
发文量
1079
审稿时长
68 days
期刊介绍:
The Journal of Thoracic and Cardiovascular Surgery presents original, peer-reviewed articles on diseases of the heart, great vessels, lungs and thorax with emphasis on surgical interventions. An official publication of The American Association for Thoracic Surgery and The Western Thoracic Surgical Association, the Journal focuses on techniques and developments in acquired cardiac surgery, congenital cardiac repair, thoracic procedures, heart and lung transplantation, mechanical circulatory support and other procedures.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


