Xiao-Wei Tang, Wen-Sen Ren, Shu Huang, Kang Zou, Huan Xu, Xiao-Min Shi, Wei Zhang, Lei Shi, Mu-Han Lü
{"title":"开发并验证用于预测肝硬化重症监护室患者院内死亡率的提名图。","authors":"Xiao-Wei Tang, Wen-Sen Ren, Shu Huang, Kang Zou, Huan Xu, Xiao-Min Shi, Wei Zhang, Lei Shi, Mu-Han Lü","doi":"10.4254/wjh.v16.i4.625","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Liver cirrhosis patients admitted to intensive care unit (ICU) have a high mortality rate.</p><p><strong>Aim: </strong>To establish and validate a nomogram for predicting in-hospital mortality of ICU patients with liver cirrhosis.</p><p><strong>Methods: </strong>We extracted demographic, etiological, vital sign, laboratory test, comorbidity, complication, treatment, and severity score data of liver cirrhosis patients from the Medical Information Mart for Intensive Care IV (MIMIC-IV) and electronic ICU (eICU) collaborative research database (eICU-CRD). Predictor selection and model building were based on the MIMIC-IV dataset. The variables selected through least absolute shrinkage and selection operator analysis were further screened through multivariate regression analysis to obtain final predictors. The final predictors were included in the multivariate logistic regression model, which was used to construct a nomogram. Finally, we conducted external validation using the eICU-CRD. The area under the receiver operating characteristic curve (AUC), decision curve, and calibration curve were used to assess the efficacy of the models.</p><p><strong>Results: </strong>Risk factors, including the mean respiratory rate, mean systolic blood pressure, mean heart rate, white blood cells, international normalized ratio, total bilirubin, age, invasive ventilation, vasopressor use, maximum stage of acute kidney injury, and sequential organ failure assessment score, were included in the multivariate logistic regression. The model achieved AUCs of 0.864 and 0.808 in the MIMIC-IV and eICU-CRD databases, respectively. The calibration curve also confirmed the predictive ability of the model, while the decision curve confirmed its clinical value.</p><p><strong>Conclusion: </strong>The nomogram has high accuracy in predicting in-hospital mortality. Improving the included predictors may help improve the prognosis of patients.</p>","PeriodicalId":23687,"journal":{"name":"World Journal of Hepatology","volume":"16 4","pages":"625-639"},"PeriodicalIF":2.5000,"publicationDate":"2024-04-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11056901/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and validation of a nomogram for predicting in-hospital mortality of intensive care unit patients with liver cirrhosis.\",\"authors\":\"Xiao-Wei Tang, Wen-Sen Ren, Shu Huang, Kang Zou, Huan Xu, Xiao-Min Shi, Wei Zhang, Lei Shi, Mu-Han Lü\",\"doi\":\"10.4254/wjh.v16.i4.625\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Liver cirrhosis patients admitted to intensive care unit (ICU) have a high mortality rate.</p><p><strong>Aim: </strong>To establish and validate a nomogram for predicting in-hospital mortality of ICU patients with liver cirrhosis.</p><p><strong>Methods: </strong>We extracted demographic, etiological, vital sign, laboratory test, comorbidity, complication, treatment, and severity score data of liver cirrhosis patients from the Medical Information Mart for Intensive Care IV (MIMIC-IV) and electronic ICU (eICU) collaborative research database (eICU-CRD). Predictor selection and model building were based on the MIMIC-IV dataset. The variables selected through least absolute shrinkage and selection operator analysis were further screened through multivariate regression analysis to obtain final predictors. The final predictors were included in the multivariate logistic regression model, which was used to construct a nomogram. Finally, we conducted external validation using the eICU-CRD. The area under the receiver operating characteristic curve (AUC), decision curve, and calibration curve were used to assess the efficacy of the models.</p><p><strong>Results: </strong>Risk factors, including the mean respiratory rate, mean systolic blood pressure, mean heart rate, white blood cells, international normalized ratio, total bilirubin, age, invasive ventilation, vasopressor use, maximum stage of acute kidney injury, and sequential organ failure assessment score, were included in the multivariate logistic regression. The model achieved AUCs of 0.864 and 0.808 in the MIMIC-IV and eICU-CRD databases, respectively. The calibration curve also confirmed the predictive ability of the model, while the decision curve confirmed its clinical value.</p><p><strong>Conclusion: </strong>The nomogram has high accuracy in predicting in-hospital mortality. Improving the included predictors may help improve the prognosis of patients.</p>\",\"PeriodicalId\":23687,\"journal\":{\"name\":\"World Journal of Hepatology\",\"volume\":\"16 4\",\"pages\":\"625-639\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-04-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11056901/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Hepatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4254/wjh.v16.i4.625\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4254/wjh.v16.i4.625","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Development and validation of a nomogram for predicting in-hospital mortality of intensive care unit patients with liver cirrhosis.
Background: Liver cirrhosis patients admitted to intensive care unit (ICU) have a high mortality rate.
Aim: To establish and validate a nomogram for predicting in-hospital mortality of ICU patients with liver cirrhosis.
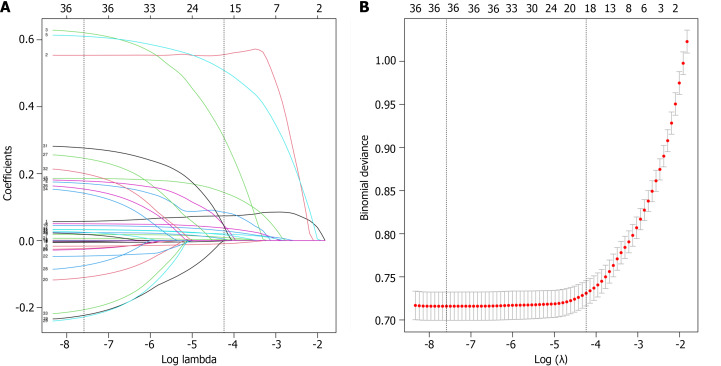
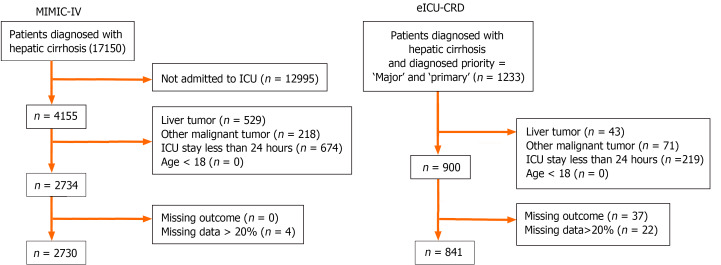
Methods: We extracted demographic, etiological, vital sign, laboratory test, comorbidity, complication, treatment, and severity score data of liver cirrhosis patients from the Medical Information Mart for Intensive Care IV (MIMIC-IV) and electronic ICU (eICU) collaborative research database (eICU-CRD). Predictor selection and model building were based on the MIMIC-IV dataset. The variables selected through least absolute shrinkage and selection operator analysis were further screened through multivariate regression analysis to obtain final predictors. The final predictors were included in the multivariate logistic regression model, which was used to construct a nomogram. Finally, we conducted external validation using the eICU-CRD. The area under the receiver operating characteristic curve (AUC), decision curve, and calibration curve were used to assess the efficacy of the models.
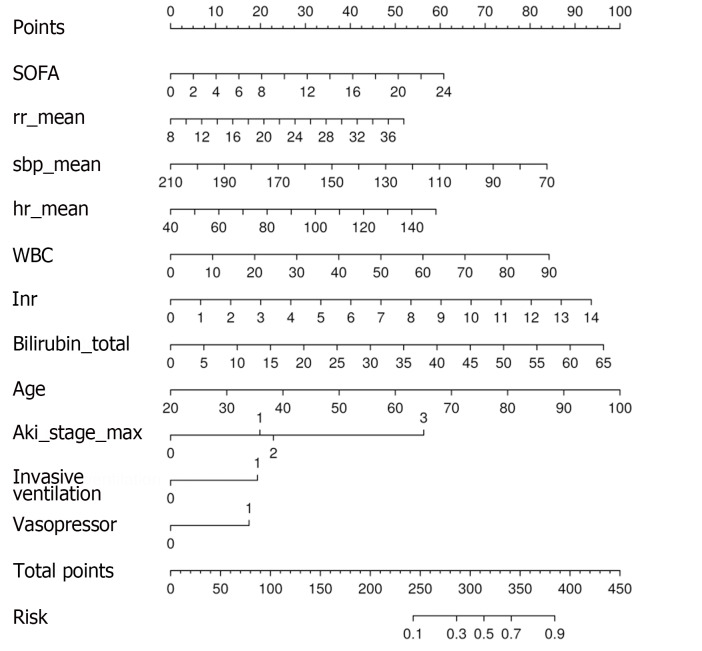
Results: Risk factors, including the mean respiratory rate, mean systolic blood pressure, mean heart rate, white blood cells, international normalized ratio, total bilirubin, age, invasive ventilation, vasopressor use, maximum stage of acute kidney injury, and sequential organ failure assessment score, were included in the multivariate logistic regression. The model achieved AUCs of 0.864 and 0.808 in the MIMIC-IV and eICU-CRD databases, respectively. The calibration curve also confirmed the predictive ability of the model, while the decision curve confirmed its clinical value.
Conclusion: The nomogram has high accuracy in predicting in-hospital mortality. Improving the included predictors may help improve the prognosis of patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


