Stephen Andrew Esper, Jennifer Holder-Murray, Katie Ann Meister, Hsing-Hua Sylvia Lin, David Kojo Hamilton, Yram Jan Groff, Brian Scott Zuckerbraun, Aman Mahajan
{"title":"新颖的数字健康平台与健康指导,优化手术患者:大型学术医疗系统的可行性研究。","authors":"Stephen Andrew Esper, Jennifer Holder-Murray, Katie Ann Meister, Hsing-Hua Sylvia Lin, David Kojo Hamilton, Yram Jan Groff, Brian Scott Zuckerbraun, Aman Mahajan","doi":"10.2196/52125","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pip is a novel digital health platform (DHP) that combines human health coaches (HCs) and technology with patient-facing content. This combination has not been studied in perioperative surgical optimization.</p><p><strong>Objective: </strong>This study's aim was to test the feasibility of the Pip platform for deploying perioperative, digital, patient-facing optimization guidelines to elective surgical patients, assisted by an HC, at predefined intervals in the perioperative journey.</p><p><strong>Methods: </strong>We conducted an institutional review board-approved, descriptive, prospective feasibility study of patients scheduled for elective surgery and invited to enroll in Pip from 2.5 to 4 weeks preoperatively through 4 weeks postoperatively at an academic medical center between November 22, 2022, and March 27, 2023. Descriptive primary end points were patient-reported outcomes, including patient satisfaction and engagement, and Pip HC evaluations. Secondary end points included mean or median length of stay (LOS), readmission at 7 and 30 days, and emergency department use within 30 days. Secondary end points were compared between patients who received Pip versus patients who did not receive Pip using stabilized inverse probability of treatment weighting.</p><p><strong>Results: </strong>A total of 283 patients were invited, of whom 172 (60.8%) enrolled in Pip. Of these, 80.2% (138/172) patients had ≥1 HC session and proceeded to surgery, and 70.3% (97/138) of the enrolled patients engaged with Pip postoperatively. The mean engagement began 27 days before surgery. Pip demonstrated an 82% weekly engagement rate with HCs. Patients attended an average of 6.7 HC sessions. Of those patients that completed surveys (95/138, 68.8%), high satisfaction scores were recorded (mean 4.8/5; n=95). Patients strongly agreed that HCs helped them throughout the perioperative process (mean 4.97/5; n=33). The average net promoter score was 9.7 out of 10. A total of 268 patients in the non-Pip group and 128 patients in the Pip group had appropriate overlapping distributions of stabilized inverse probability of treatment weighting for the analytic sample. The Pip cohort was associated with LOS reduction when compared to the non-Pip cohort (mean 2.4 vs 3.1 days; median 1.9, IQR 1.0-3.1 vs median 3.0, IQR 1.1-3.9 days; mean ratio 0.76; 95% CI 0.62-0.93; P=.009). The Pip cohort experienced a 49% lower risk of 7-day readmission (relative risk [RR] 0.51, 95% CI 0.11-2.31; P=.38) and a 17% lower risk of 30-day readmission (RR 0.83, 95% CI 0.30-2.31; P=.73), though these did not reach statistical significance. Both cohorts had similar 30-day emergency department returns (RR 1.06, 95% CI 0.56-2.01, P=.85).</p><p><strong>Conclusions: </strong>Pip is a novel mobile DHP combining human HCs and perioperative optimization content that is feasible to engage patients in their perioperative journey and is associated with reduced hospital LOS. Further studies assessing the impact on clinical and patient-reported outcomes from the use of Pip or similar DHPs HC combinations during the perioperative journey are required.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"7 ","pages":"e52125"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11027047/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Novel Digital Health Platform With Health Coaches to Optimize Surgical Patients: Feasibility Study at a Large Academic Health System.\",\"authors\":\"Stephen Andrew Esper, Jennifer Holder-Murray, Katie Ann Meister, Hsing-Hua Sylvia Lin, David Kojo Hamilton, Yram Jan Groff, Brian Scott Zuckerbraun, Aman Mahajan\",\"doi\":\"10.2196/52125\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pip is a novel digital health platform (DHP) that combines human health coaches (HCs) and technology with patient-facing content. This combination has not been studied in perioperative surgical optimization.</p><p><strong>Objective: </strong>This study's aim was to test the feasibility of the Pip platform for deploying perioperative, digital, patient-facing optimization guidelines to elective surgical patients, assisted by an HC, at predefined intervals in the perioperative journey.</p><p><strong>Methods: </strong>We conducted an institutional review board-approved, descriptive, prospective feasibility study of patients scheduled for elective surgery and invited to enroll in Pip from 2.5 to 4 weeks preoperatively through 4 weeks postoperatively at an academic medical center between November 22, 2022, and March 27, 2023. Descriptive primary end points were patient-reported outcomes, including patient satisfaction and engagement, and Pip HC evaluations. Secondary end points included mean or median length of stay (LOS), readmission at 7 and 30 days, and emergency department use within 30 days. Secondary end points were compared between patients who received Pip versus patients who did not receive Pip using stabilized inverse probability of treatment weighting.</p><p><strong>Results: </strong>A total of 283 patients were invited, of whom 172 (60.8%) enrolled in Pip. Of these, 80.2% (138/172) patients had ≥1 HC session and proceeded to surgery, and 70.3% (97/138) of the enrolled patients engaged with Pip postoperatively. The mean engagement began 27 days before surgery. Pip demonstrated an 82% weekly engagement rate with HCs. Patients attended an average of 6.7 HC sessions. Of those patients that completed surveys (95/138, 68.8%), high satisfaction scores were recorded (mean 4.8/5; n=95). Patients strongly agreed that HCs helped them throughout the perioperative process (mean 4.97/5; n=33). The average net promoter score was 9.7 out of 10. A total of 268 patients in the non-Pip group and 128 patients in the Pip group had appropriate overlapping distributions of stabilized inverse probability of treatment weighting for the analytic sample. The Pip cohort was associated with LOS reduction when compared to the non-Pip cohort (mean 2.4 vs 3.1 days; median 1.9, IQR 1.0-3.1 vs median 3.0, IQR 1.1-3.9 days; mean ratio 0.76; 95% CI 0.62-0.93; P=.009). The Pip cohort experienced a 49% lower risk of 7-day readmission (relative risk [RR] 0.51, 95% CI 0.11-2.31; P=.38) and a 17% lower risk of 30-day readmission (RR 0.83, 95% CI 0.30-2.31; P=.73), though these did not reach statistical significance. Both cohorts had similar 30-day emergency department returns (RR 1.06, 95% CI 0.56-2.01, P=.85).</p><p><strong>Conclusions: </strong>Pip is a novel mobile DHP combining human HCs and perioperative optimization content that is feasible to engage patients in their perioperative journey and is associated with reduced hospital LOS. Further studies assessing the impact on clinical and patient-reported outcomes from the use of Pip or similar DHPs HC combinations during the perioperative journey are required.</p>\",\"PeriodicalId\":73557,\"journal\":{\"name\":\"JMIR perioperative medicine\",\"volume\":\"7 \",\"pages\":\"e52125\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-04-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11027047/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR perioperative medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/52125\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/52125","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A Novel Digital Health Platform With Health Coaches to Optimize Surgical Patients: Feasibility Study at a Large Academic Health System.
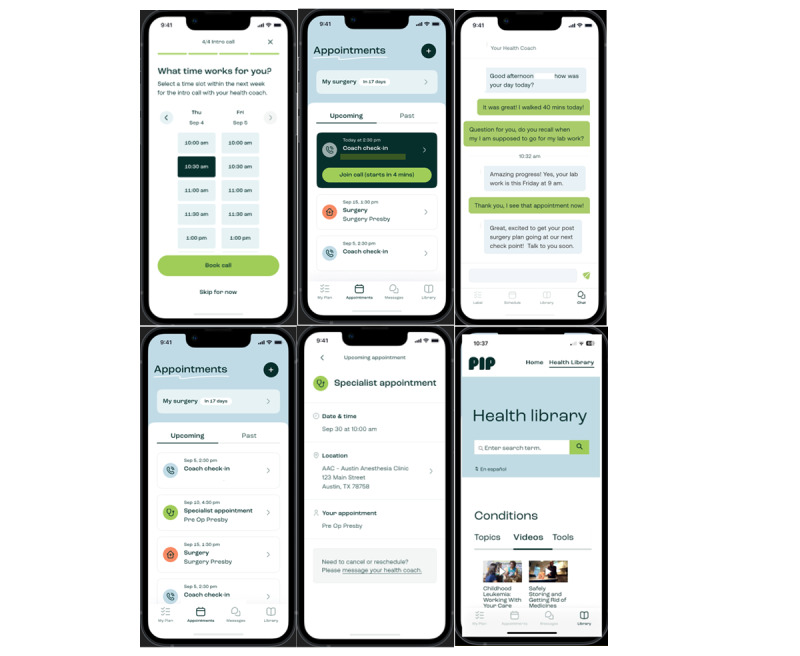
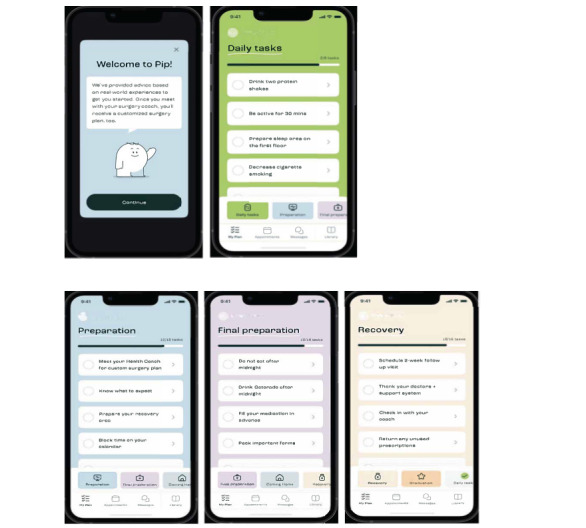
Background: Pip is a novel digital health platform (DHP) that combines human health coaches (HCs) and technology with patient-facing content. This combination has not been studied in perioperative surgical optimization.
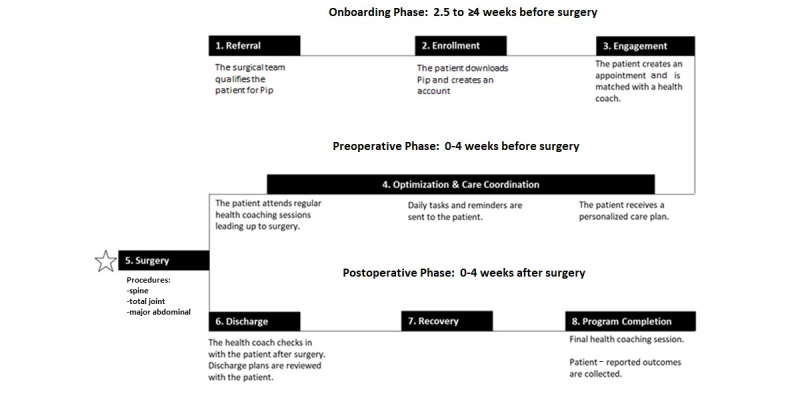
Objective: This study's aim was to test the feasibility of the Pip platform for deploying perioperative, digital, patient-facing optimization guidelines to elective surgical patients, assisted by an HC, at predefined intervals in the perioperative journey.
Methods: We conducted an institutional review board-approved, descriptive, prospective feasibility study of patients scheduled for elective surgery and invited to enroll in Pip from 2.5 to 4 weeks preoperatively through 4 weeks postoperatively at an academic medical center between November 22, 2022, and March 27, 2023. Descriptive primary end points were patient-reported outcomes, including patient satisfaction and engagement, and Pip HC evaluations. Secondary end points included mean or median length of stay (LOS), readmission at 7 and 30 days, and emergency department use within 30 days. Secondary end points were compared between patients who received Pip versus patients who did not receive Pip using stabilized inverse probability of treatment weighting.
Results: A total of 283 patients were invited, of whom 172 (60.8%) enrolled in Pip. Of these, 80.2% (138/172) patients had ≥1 HC session and proceeded to surgery, and 70.3% (97/138) of the enrolled patients engaged with Pip postoperatively. The mean engagement began 27 days before surgery. Pip demonstrated an 82% weekly engagement rate with HCs. Patients attended an average of 6.7 HC sessions. Of those patients that completed surveys (95/138, 68.8%), high satisfaction scores were recorded (mean 4.8/5; n=95). Patients strongly agreed that HCs helped them throughout the perioperative process (mean 4.97/5; n=33). The average net promoter score was 9.7 out of 10. A total of 268 patients in the non-Pip group and 128 patients in the Pip group had appropriate overlapping distributions of stabilized inverse probability of treatment weighting for the analytic sample. The Pip cohort was associated with LOS reduction when compared to the non-Pip cohort (mean 2.4 vs 3.1 days; median 1.9, IQR 1.0-3.1 vs median 3.0, IQR 1.1-3.9 days; mean ratio 0.76; 95% CI 0.62-0.93; P=.009). The Pip cohort experienced a 49% lower risk of 7-day readmission (relative risk [RR] 0.51, 95% CI 0.11-2.31; P=.38) and a 17% lower risk of 30-day readmission (RR 0.83, 95% CI 0.30-2.31; P=.73), though these did not reach statistical significance. Both cohorts had similar 30-day emergency department returns (RR 1.06, 95% CI 0.56-2.01, P=.85).
Conclusions: Pip is a novel mobile DHP combining human HCs and perioperative optimization content that is feasible to engage patients in their perioperative journey and is associated with reduced hospital LOS. Further studies assessing the impact on clinical and patient-reported outcomes from the use of Pip or similar DHPs HC combinations during the perioperative journey are required.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


