{"title":"减少四级新生儿重症监护室中与早产儿相关骨折的骨质疏松:质量改进计划。","authors":"Linsey Cromwell, Katherine Breznak, Megan Young, Anoosha Kasangottu, Sharon Leonardo, Catherine Markel, Andreea Marinescu, Folasade Kehinde, Vilmaris Quinones Cardona","doi":"10.1097/pq9.0000000000000723","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Osteopenia of prematurity (OOP) is often a silent disease in the neonatal intensive care unit (NICU). Despite its association with increased neonatal morbidity, such as fractures, wide variation exists in screening, diagnostic, and management practices. We sought to decrease the rate of OOP-related fractures in our level IV NICU by 20% within 1 year.</p><p><strong>Methods: </strong>A multidisciplinary quality improvement team identified inconsistent screening, diagnosis, and management of OOP, as well as handling of at-risk patients, as primary drivers for OOP-related fractures. Using the model for improvement, we implemented sequential interventions, including screening, diagnosis, and a management algorithm as a \"handle-with-care\" bundle in infants at risk for fractures.</p><p><strong>Results: </strong>194 at-risk infants were included, 59 of whom had OOP. There was special cause variation in OOP-related fractures, with a reduction from 0.43 per 1000 patient days to 0.06 per 1000 patient days with our interventions. There was also an improvement in days between fractures from 62 to 337 days. We achieved these improvements despite a similar prevalence of OOP throughout the initiative. We showed special cause variation with increased patients between missed OOP documentation and improved collection of OOP screening laboratories at 4 weeks of life without increased blood testing.</p><p><strong>Conclusion: </strong>A multidisciplinary team approach with standardized OOP screening, diagnosis, and management guidelines, including a handle-with-care bundle, reduces OOP-related fractures in a level IV NICU.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 2","pages":"e723"},"PeriodicalIF":1.1000,"publicationDate":"2024-04-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10990331/pdf/","citationCount":"0","resultStr":"{\"title\":\"Reducing Osteopenia of Prematurity-related Fractures in a Level IV NICU: A Quality Improvement Initiative.\",\"authors\":\"Linsey Cromwell, Katherine Breznak, Megan Young, Anoosha Kasangottu, Sharon Leonardo, Catherine Markel, Andreea Marinescu, Folasade Kehinde, Vilmaris Quinones Cardona\",\"doi\":\"10.1097/pq9.0000000000000723\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Osteopenia of prematurity (OOP) is often a silent disease in the neonatal intensive care unit (NICU). Despite its association with increased neonatal morbidity, such as fractures, wide variation exists in screening, diagnostic, and management practices. We sought to decrease the rate of OOP-related fractures in our level IV NICU by 20% within 1 year.</p><p><strong>Methods: </strong>A multidisciplinary quality improvement team identified inconsistent screening, diagnosis, and management of OOP, as well as handling of at-risk patients, as primary drivers for OOP-related fractures. Using the model for improvement, we implemented sequential interventions, including screening, diagnosis, and a management algorithm as a \\\"handle-with-care\\\" bundle in infants at risk for fractures.</p><p><strong>Results: </strong>194 at-risk infants were included, 59 of whom had OOP. There was special cause variation in OOP-related fractures, with a reduction from 0.43 per 1000 patient days to 0.06 per 1000 patient days with our interventions. There was also an improvement in days between fractures from 62 to 337 days. We achieved these improvements despite a similar prevalence of OOP throughout the initiative. We showed special cause variation with increased patients between missed OOP documentation and improved collection of OOP screening laboratories at 4 weeks of life without increased blood testing.</p><p><strong>Conclusion: </strong>A multidisciplinary team approach with standardized OOP screening, diagnosis, and management guidelines, including a handle-with-care bundle, reduces OOP-related fractures in a level IV NICU.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"9 2\",\"pages\":\"e723\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-04-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10990331/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000723\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000723","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Reducing Osteopenia of Prematurity-related Fractures in a Level IV NICU: A Quality Improvement Initiative.
Background: Osteopenia of prematurity (OOP) is often a silent disease in the neonatal intensive care unit (NICU). Despite its association with increased neonatal morbidity, such as fractures, wide variation exists in screening, diagnostic, and management practices. We sought to decrease the rate of OOP-related fractures in our level IV NICU by 20% within 1 year.
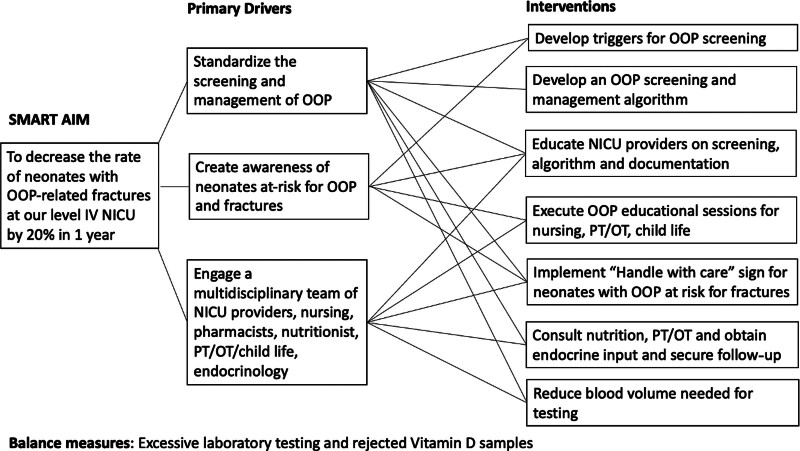
Methods: A multidisciplinary quality improvement team identified inconsistent screening, diagnosis, and management of OOP, as well as handling of at-risk patients, as primary drivers for OOP-related fractures. Using the model for improvement, we implemented sequential interventions, including screening, diagnosis, and a management algorithm as a "handle-with-care" bundle in infants at risk for fractures.
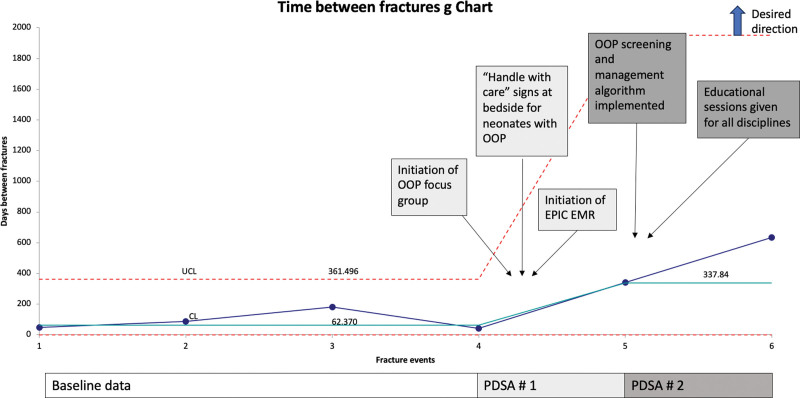
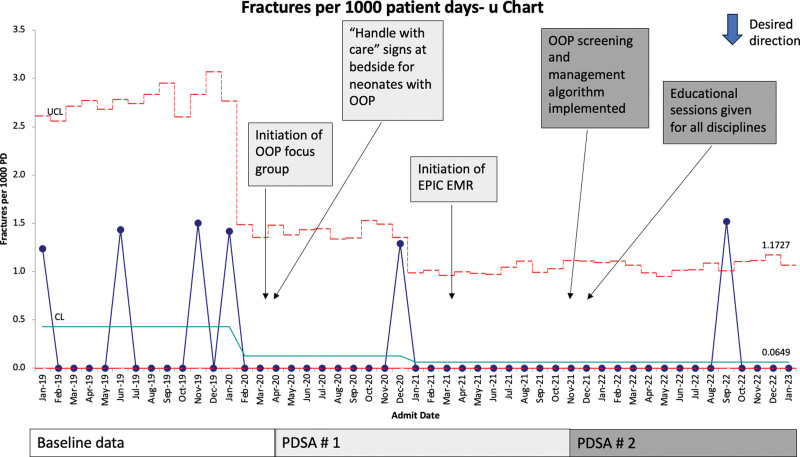
Results: 194 at-risk infants were included, 59 of whom had OOP. There was special cause variation in OOP-related fractures, with a reduction from 0.43 per 1000 patient days to 0.06 per 1000 patient days with our interventions. There was also an improvement in days between fractures from 62 to 337 days. We achieved these improvements despite a similar prevalence of OOP throughout the initiative. We showed special cause variation with increased patients between missed OOP documentation and improved collection of OOP screening laboratories at 4 weeks of life without increased blood testing.
Conclusion: A multidisciplinary team approach with standardized OOP screening, diagnosis, and management guidelines, including a handle-with-care bundle, reduces OOP-related fractures in a level IV NICU.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


