Katrine Fjaellegaard, Jesper Koefod Petersen, Gitte Alstrup, Søren Skaarup, Paul Frost Clementsen, Christian B Laursen, Rahul Bhatnagar, Uffe Bodtger
{"title":"超声波预测复发性单侧胸腔积液患者治疗性胸腔穿刺术后呼吸困难的改善情况。","authors":"Katrine Fjaellegaard, Jesper Koefod Petersen, Gitte Alstrup, Søren Skaarup, Paul Frost Clementsen, Christian B Laursen, Rahul Bhatnagar, Uffe Bodtger","doi":"10.1080/20018525.2024.2337446","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with recurrent pleural effusion, therapeutic thoracentesis is one way of relief. Correct prediction of which patients will experience relief following drainage may support the management of these patients. This study aimed to assess the association between ultrasound (US) characteristics and a relevant improvement in dyspnoea immediately following drainage.</p><p><strong>Methods: </strong>In a prospective, observational study, patients with recurrent unilateral pleural effusion underwent US evaluation of effusion characteristics and diaphragm movement measured by M-mode and the Area method before and right after drainage. The level of dyspnoea was assessed using the modified Borg scale (MBS). A minimal important improvement in dyspnoea was defined as delta MBS ≥ 1.</p><p><strong>Results: </strong>In the 104 patients included, 53% had a minimal important improvement in dyspnoea following thoracentesis. We found no association between US-characteristics, including diaphragm shape or movement (M-mode or the Area method), and a decrease in dyspnoea following drainage. Baseline MBS score ≥ 4 and a fully drained effusion were significant correlated with a minimal important improvement in dyspnoea (OR 3.86 (1.42-10.50), <i>p</i> = 0.01 and 2.86 (1.03-7.93), <i>p</i> = 0.04, respectively).</p><p><strong>Conclusions: </strong>In our study population, US-characteristics including assessment of diaphragm movement or shape was not associated with a minimal important improvement in dyspnoea immediately following thoracentesis.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"11 1","pages":"2337446"},"PeriodicalIF":1.4000,"publicationDate":"2024-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11073413/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ultrasound in predicting improvement in dyspnoea after therapeutic thoracentesis in patients with recurrent unilateral pleural effusion.\",\"authors\":\"Katrine Fjaellegaard, Jesper Koefod Petersen, Gitte Alstrup, Søren Skaarup, Paul Frost Clementsen, Christian B Laursen, Rahul Bhatnagar, Uffe Bodtger\",\"doi\":\"10.1080/20018525.2024.2337446\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In patients with recurrent pleural effusion, therapeutic thoracentesis is one way of relief. Correct prediction of which patients will experience relief following drainage may support the management of these patients. This study aimed to assess the association between ultrasound (US) characteristics and a relevant improvement in dyspnoea immediately following drainage.</p><p><strong>Methods: </strong>In a prospective, observational study, patients with recurrent unilateral pleural effusion underwent US evaluation of effusion characteristics and diaphragm movement measured by M-mode and the Area method before and right after drainage. The level of dyspnoea was assessed using the modified Borg scale (MBS). A minimal important improvement in dyspnoea was defined as delta MBS ≥ 1.</p><p><strong>Results: </strong>In the 104 patients included, 53% had a minimal important improvement in dyspnoea following thoracentesis. We found no association between US-characteristics, including diaphragm shape or movement (M-mode or the Area method), and a decrease in dyspnoea following drainage. Baseline MBS score ≥ 4 and a fully drained effusion were significant correlated with a minimal important improvement in dyspnoea (OR 3.86 (1.42-10.50), <i>p</i> = 0.01 and 2.86 (1.03-7.93), <i>p</i> = 0.04, respectively).</p><p><strong>Conclusions: </strong>In our study population, US-characteristics including assessment of diaphragm movement or shape was not associated with a minimal important improvement in dyspnoea immediately following thoracentesis.</p>\",\"PeriodicalId\":11872,\"journal\":{\"name\":\"European Clinical Respiratory Journal\",\"volume\":\"11 1\",\"pages\":\"2337446\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-05-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11073413/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Clinical Respiratory Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20018525.2024.2337446\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2024.2337446","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
背景:对于复发性胸腔积液患者,治疗性胸腔穿刺术是一种缓解方法。正确预测哪些患者在引流后症状会得到缓解,有助于这些患者的治疗。本研究旨在评估超声(US)特征与引流后呼吸困难立即得到改善之间的关联:在一项前瞻性观察研究中,复发性单侧胸腔积液患者在引流前和引流后立即接受了超声评估,通过 M 型和面积法测量了积液特征和横膈膜运动。呼吸困难程度采用改良博格量表(MBS)进行评估。结果:在纳入的 104 名患者中,53% 的患者在胸腔穿刺术后呼吸困难得到了最小程度的改善。我们发现 US 特征(包括横膈膜形状或移动(M 模式或区域法))与引流后呼吸困难的减轻之间没有关联。基线 MBS 评分≥4 和完全引流的积液与呼吸困难的最小重要改善显著相关(OR 分别为 3.86 (1.42-10.50),p = 0.01 和 2.86 (1.03-7.93),p = 0.04):在我们的研究人群中,包括评估横膈膜运动或形状在内的 US 特征与胸腔穿刺术后呼吸困难的最小重要改善无关。
Ultrasound in predicting improvement in dyspnoea after therapeutic thoracentesis in patients with recurrent unilateral pleural effusion.
Background: In patients with recurrent pleural effusion, therapeutic thoracentesis is one way of relief. Correct prediction of which patients will experience relief following drainage may support the management of these patients. This study aimed to assess the association between ultrasound (US) characteristics and a relevant improvement in dyspnoea immediately following drainage.
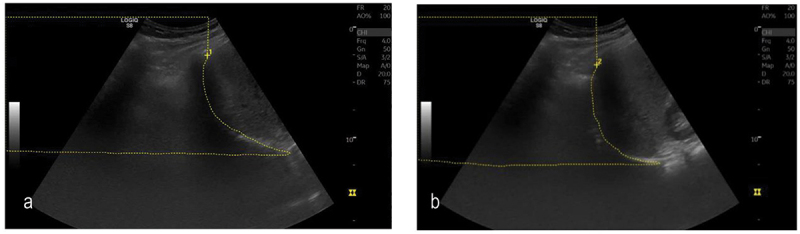
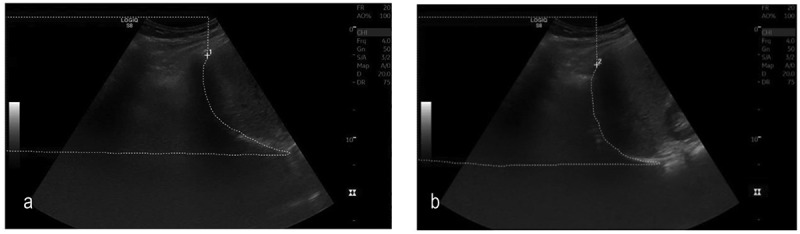
Methods: In a prospective, observational study, patients with recurrent unilateral pleural effusion underwent US evaluation of effusion characteristics and diaphragm movement measured by M-mode and the Area method before and right after drainage. The level of dyspnoea was assessed using the modified Borg scale (MBS). A minimal important improvement in dyspnoea was defined as delta MBS ≥ 1.
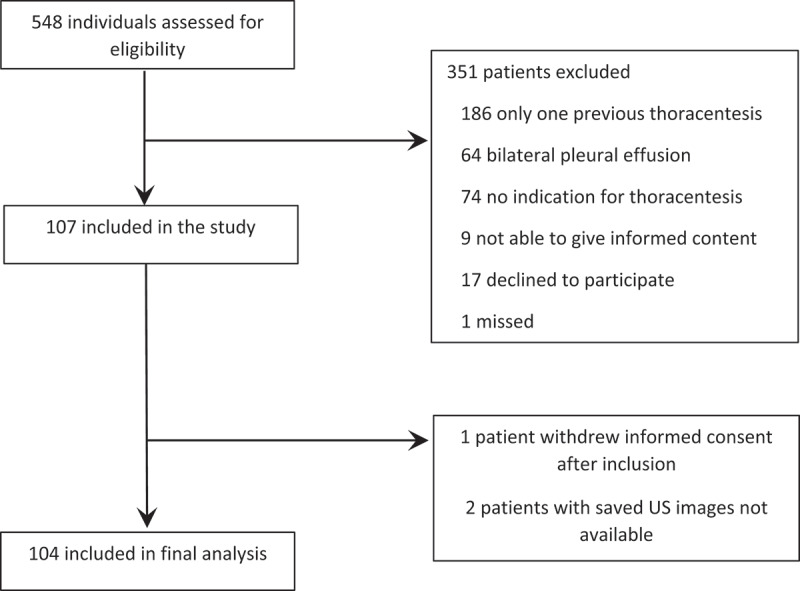
Results: In the 104 patients included, 53% had a minimal important improvement in dyspnoea following thoracentesis. We found no association between US-characteristics, including diaphragm shape or movement (M-mode or the Area method), and a decrease in dyspnoea following drainage. Baseline MBS score ≥ 4 and a fully drained effusion were significant correlated with a minimal important improvement in dyspnoea (OR 3.86 (1.42-10.50), p = 0.01 and 2.86 (1.03-7.93), p = 0.04, respectively).
Conclusions: In our study population, US-characteristics including assessment of diaphragm movement or shape was not associated with a minimal important improvement in dyspnoea immediately following thoracentesis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


