Turky Arbaein, Bert Little, Sarah Monshi, Ahmed M Al-Wathinani, Amal Zaidan
{"title":"医疗补助计划扩展前后肯塔基州 2 型糖尿病患者可预防住院治疗的变化。","authors":"Turky Arbaein, Bert Little, Sarah Monshi, Ahmed M Al-Wathinani, Amal Zaidan","doi":"10.5144/0256-4947.2024.73","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hospitalizations are more resource intensive and expensive than outpatient care. Therefore, type 2 diabetes-related preventable hospitalization are a major topic of research efficiency in the healthcare system.</p><p><strong>Objectives: </strong>Analyze county level variation in type 2 diabetes-related preventable hospitalization rates in Kentucky before the Medicaid expansion (2010-2013) and after the Medicaid expansion (2014-2017).</p><p><strong>Design: </strong>Geographic mapping and cluster analysis.</p><p><strong>Setting: </strong>Data for a state of the United States of America.</p><p><strong>Methods: </strong>We used the KID data to generate geographic mapping for type 2 diabetes-related preventable hospitalizations to visualize rates. We included all Kentucky discharges of age 18 years and older with the ICD9/10 principal diagnosis code for type 2 diabetes. Then, we conducted cluster analysis techniques to compare county-level variation in type 2 diabetes-related preventable hospitalization rates across Kentucky counties pre- and post-Medicaid expansion.</p><p><strong>Main outcome and measures: </strong>County type 2 diabetes-related preventable hospitalization pre- and post-Medicaid expansion.</p><p><strong>Results: </strong>From 2010-2017, type 2 diabetes-related preventable hospitalization discharge rates reduced significantly in the period of the post-Medicaid expansion (<i>P</i>=.001). The spatial statistics analysis revealed a significant spatial clustering of counties with similar rates of type 2 diabetes-related preventable hospitalization in the south, east, and southeastern Kentucky pre- and post-Medicaid expansion (positive z-score and positive Moran's Index value (<i>P</i>>.05). Also, there was a significant clustering of counties with low type 2 diabetes-related preventable hospitalization rates in the north, west, and central regions of the state pre-Medicaid expansion and post-Medicaid expansion (positive z-score and positive Moran's Index value (<i>P</i>>.05).</p><p><strong>Conclusion: </strong>Kentucky counties in the southeast have experienced a significant clustering of highly avoidable hospitalization rates during both periods. Focusing on the vulnerable counties and the economic inequality in Kentucky could lead to efforts to lowering future type 2 diabetes-related preventable hospitalization rates.</p><p><strong>Limitations: </strong>We used de-identified data which does not provide insights into the frequency of hospitalizations per patient. An individual patient may be hospitalized several times and counted as several individuals.</p>","PeriodicalId":93875,"journal":{"name":"Annals of Saudi medicine","volume":"44 2","pages":"73-83"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11016150/pdf/","citationCount":"0","resultStr":"{\"title\":\"The variation in preventable hospitalization in patients with type 2 diabetes in Kentucky before and after the Medicaid expansion.\",\"authors\":\"Turky Arbaein, Bert Little, Sarah Monshi, Ahmed M Al-Wathinani, Amal Zaidan\",\"doi\":\"10.5144/0256-4947.2024.73\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hospitalizations are more resource intensive and expensive than outpatient care. Therefore, type 2 diabetes-related preventable hospitalization are a major topic of research efficiency in the healthcare system.</p><p><strong>Objectives: </strong>Analyze county level variation in type 2 diabetes-related preventable hospitalization rates in Kentucky before the Medicaid expansion (2010-2013) and after the Medicaid expansion (2014-2017).</p><p><strong>Design: </strong>Geographic mapping and cluster analysis.</p><p><strong>Setting: </strong>Data for a state of the United States of America.</p><p><strong>Methods: </strong>We used the KID data to generate geographic mapping for type 2 diabetes-related preventable hospitalizations to visualize rates. We included all Kentucky discharges of age 18 years and older with the ICD9/10 principal diagnosis code for type 2 diabetes. Then, we conducted cluster analysis techniques to compare county-level variation in type 2 diabetes-related preventable hospitalization rates across Kentucky counties pre- and post-Medicaid expansion.</p><p><strong>Main outcome and measures: </strong>County type 2 diabetes-related preventable hospitalization pre- and post-Medicaid expansion.</p><p><strong>Results: </strong>From 2010-2017, type 2 diabetes-related preventable hospitalization discharge rates reduced significantly in the period of the post-Medicaid expansion (<i>P</i>=.001). The spatial statistics analysis revealed a significant spatial clustering of counties with similar rates of type 2 diabetes-related preventable hospitalization in the south, east, and southeastern Kentucky pre- and post-Medicaid expansion (positive z-score and positive Moran's Index value (<i>P</i>>.05). Also, there was a significant clustering of counties with low type 2 diabetes-related preventable hospitalization rates in the north, west, and central regions of the state pre-Medicaid expansion and post-Medicaid expansion (positive z-score and positive Moran's Index value (<i>P</i>>.05).</p><p><strong>Conclusion: </strong>Kentucky counties in the southeast have experienced a significant clustering of highly avoidable hospitalization rates during both periods. Focusing on the vulnerable counties and the economic inequality in Kentucky could lead to efforts to lowering future type 2 diabetes-related preventable hospitalization rates.</p><p><strong>Limitations: </strong>We used de-identified data which does not provide insights into the frequency of hospitalizations per patient. An individual patient may be hospitalized several times and counted as several individuals.</p>\",\"PeriodicalId\":93875,\"journal\":{\"name\":\"Annals of Saudi medicine\",\"volume\":\"44 2\",\"pages\":\"73-83\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11016150/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Saudi medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5144/0256-4947.2024.73\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/4/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Saudi medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5144/0256-4947.2024.73","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/4 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
The variation in preventable hospitalization in patients with type 2 diabetes in Kentucky before and after the Medicaid expansion.
Background: Hospitalizations are more resource intensive and expensive than outpatient care. Therefore, type 2 diabetes-related preventable hospitalization are a major topic of research efficiency in the healthcare system.
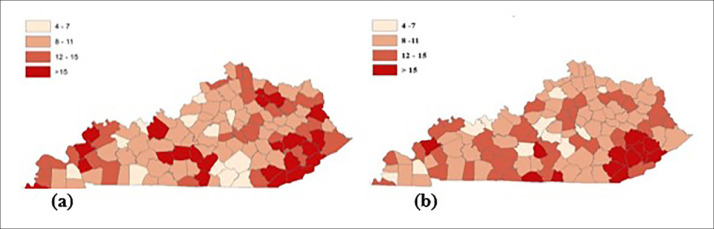
Objectives: Analyze county level variation in type 2 diabetes-related preventable hospitalization rates in Kentucky before the Medicaid expansion (2010-2013) and after the Medicaid expansion (2014-2017).
Design: Geographic mapping and cluster analysis.
Setting: Data for a state of the United States of America.
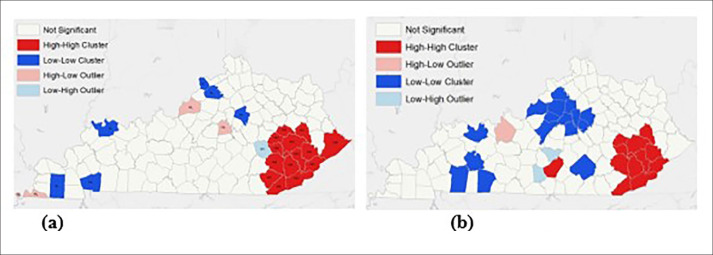
Methods: We used the KID data to generate geographic mapping for type 2 diabetes-related preventable hospitalizations to visualize rates. We included all Kentucky discharges of age 18 years and older with the ICD9/10 principal diagnosis code for type 2 diabetes. Then, we conducted cluster analysis techniques to compare county-level variation in type 2 diabetes-related preventable hospitalization rates across Kentucky counties pre- and post-Medicaid expansion.
Main outcome and measures: County type 2 diabetes-related preventable hospitalization pre- and post-Medicaid expansion.
Results: From 2010-2017, type 2 diabetes-related preventable hospitalization discharge rates reduced significantly in the period of the post-Medicaid expansion (P=.001). The spatial statistics analysis revealed a significant spatial clustering of counties with similar rates of type 2 diabetes-related preventable hospitalization in the south, east, and southeastern Kentucky pre- and post-Medicaid expansion (positive z-score and positive Moran's Index value (P>.05). Also, there was a significant clustering of counties with low type 2 diabetes-related preventable hospitalization rates in the north, west, and central regions of the state pre-Medicaid expansion and post-Medicaid expansion (positive z-score and positive Moran's Index value (P>.05).
Conclusion: Kentucky counties in the southeast have experienced a significant clustering of highly avoidable hospitalization rates during both periods. Focusing on the vulnerable counties and the economic inequality in Kentucky could lead to efforts to lowering future type 2 diabetes-related preventable hospitalization rates.
Limitations: We used de-identified data which does not provide insights into the frequency of hospitalizations per patient. An individual patient may be hospitalized several times and counted as several individuals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


