Stephanie N Chen, Jessica B Holstine, Julie Balch Samora
{"title":"减少幼儿骨折的硬性固定:质量改进计划。","authors":"Stephanie N Chen, Jessica B Holstine, Julie Balch Samora","doi":"10.1097/pq9.0000000000000722","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Toddler's fractures are one of the most common orthopedic injuries in young walking-age children. They are defined as nondisplaced spiral-type metaphyseal fractures involving only the tibia without any injury to the fibula and are inherently stable. We aimed to use quality improvement methodology to increase the proportion of patients with toddler's fractures treated without cast immobilization at a large tertiary referral pediatric orthopedic center from a baseline of 45.6%-75%.</p><p><strong>Methods: </strong>Baseline data on patient volume and treatment regimens for toddler's fractures were collected starting in February 2019. Monthly data were collected from the electronic medical record and reviewed to determine treatment (cast versus noncast immobilization) and tracked using statistical process control charts (p-chart). After determining the root causes of treatment using immobilization, interventions tested and adopted included physician alignment of expectations for treatment, sharing unblinded compliance data with providers, updating patient education materials, and updating resident education and reference materials.</p><p><strong>Results: </strong>After interventions were in place, the percentage of patients treated without CAST immobilization increased from 45.6% to 90% (<i>P</i> ≤ 0.001). We also observed improvement in our process measure to increase the percentage of this population receiving boot immobilization during new patient visits in our orthopedic clinics (4.15% to 52%, <i>P</i> ≤ 0.001).</p><p><strong>Conclusions: </strong>By aligning provider and family expectations for treatment, demonstrating no clinical need for cast immobilization, and bringing awareness of compliance to appropriate guidelines, our institution was able to improve care for patients with toddler's fractures and reduce financial and care burdens for families.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 2","pages":"e722"},"PeriodicalIF":1.1000,"publicationDate":"2024-04-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10990314/pdf/","citationCount":"0","resultStr":"{\"title\":\"Reducing Rigid Immobilization for Toddler's Fractures: A Quality Improvement Initiative.\",\"authors\":\"Stephanie N Chen, Jessica B Holstine, Julie Balch Samora\",\"doi\":\"10.1097/pq9.0000000000000722\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Toddler's fractures are one of the most common orthopedic injuries in young walking-age children. They are defined as nondisplaced spiral-type metaphyseal fractures involving only the tibia without any injury to the fibula and are inherently stable. We aimed to use quality improvement methodology to increase the proportion of patients with toddler's fractures treated without cast immobilization at a large tertiary referral pediatric orthopedic center from a baseline of 45.6%-75%.</p><p><strong>Methods: </strong>Baseline data on patient volume and treatment regimens for toddler's fractures were collected starting in February 2019. Monthly data were collected from the electronic medical record and reviewed to determine treatment (cast versus noncast immobilization) and tracked using statistical process control charts (p-chart). After determining the root causes of treatment using immobilization, interventions tested and adopted included physician alignment of expectations for treatment, sharing unblinded compliance data with providers, updating patient education materials, and updating resident education and reference materials.</p><p><strong>Results: </strong>After interventions were in place, the percentage of patients treated without CAST immobilization increased from 45.6% to 90% (<i>P</i> ≤ 0.001). We also observed improvement in our process measure to increase the percentage of this population receiving boot immobilization during new patient visits in our orthopedic clinics (4.15% to 52%, <i>P</i> ≤ 0.001).</p><p><strong>Conclusions: </strong>By aligning provider and family expectations for treatment, demonstrating no clinical need for cast immobilization, and bringing awareness of compliance to appropriate guidelines, our institution was able to improve care for patients with toddler's fractures and reduce financial and care burdens for families.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"9 2\",\"pages\":\"e722\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-04-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10990314/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000722\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000722","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Reducing Rigid Immobilization for Toddler's Fractures: A Quality Improvement Initiative.
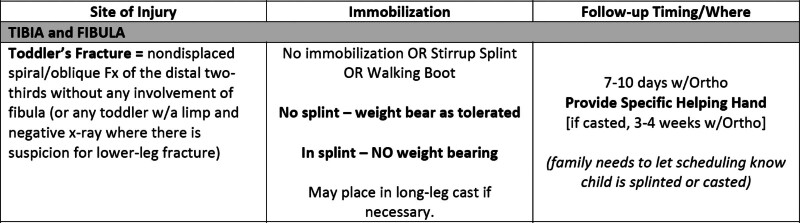
Background: Toddler's fractures are one of the most common orthopedic injuries in young walking-age children. They are defined as nondisplaced spiral-type metaphyseal fractures involving only the tibia without any injury to the fibula and are inherently stable. We aimed to use quality improvement methodology to increase the proportion of patients with toddler's fractures treated without cast immobilization at a large tertiary referral pediatric orthopedic center from a baseline of 45.6%-75%.
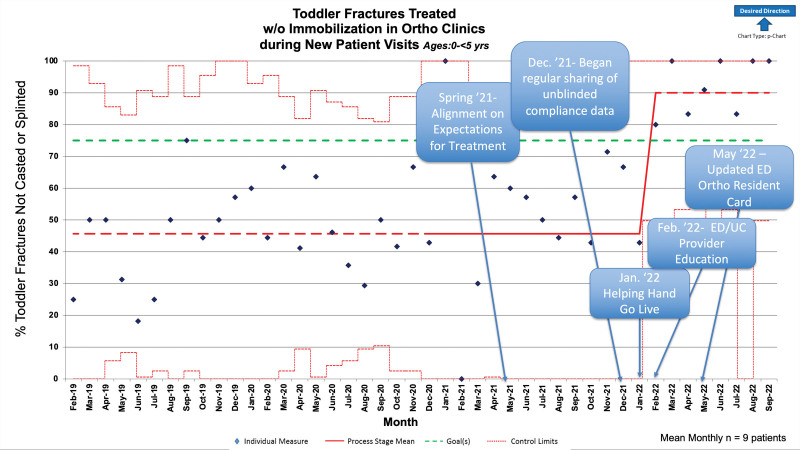
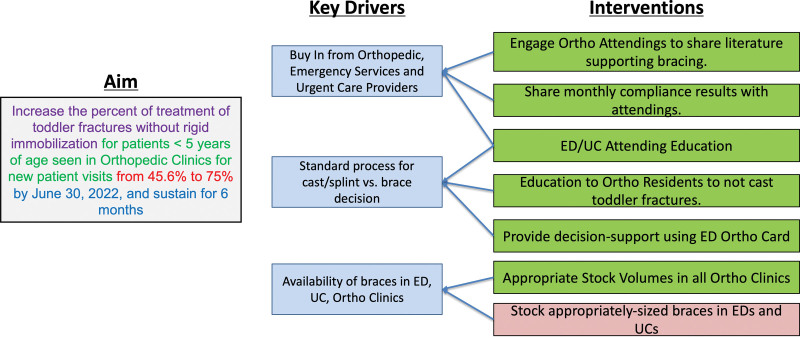
Methods: Baseline data on patient volume and treatment regimens for toddler's fractures were collected starting in February 2019. Monthly data were collected from the electronic medical record and reviewed to determine treatment (cast versus noncast immobilization) and tracked using statistical process control charts (p-chart). After determining the root causes of treatment using immobilization, interventions tested and adopted included physician alignment of expectations for treatment, sharing unblinded compliance data with providers, updating patient education materials, and updating resident education and reference materials.
Results: After interventions were in place, the percentage of patients treated without CAST immobilization increased from 45.6% to 90% (P ≤ 0.001). We also observed improvement in our process measure to increase the percentage of this population receiving boot immobilization during new patient visits in our orthopedic clinics (4.15% to 52%, P ≤ 0.001).
Conclusions: By aligning provider and family expectations for treatment, demonstrating no clinical need for cast immobilization, and bringing awareness of compliance to appropriate guidelines, our institution was able to improve care for patients with toddler's fractures and reduce financial and care burdens for families.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


