Constance Owens-Jasey, Jinying Chen, Ran Xu, Heather Angier, Amy G Huebschmann, Mayuko Ito Fukunaga, Krisda H Chaiyachati, Katharine A Rendle, Kim Robien, Lisa DiMartino, Daniel J Amante, Jamie M Faro, Maura M Kepper, Alex T Ramsey, Eric Bressman, Rachel Gold
{"title":"在美国初级保健中实施用于癌症筛查的医疗信息技术:范围审查。","authors":"Constance Owens-Jasey, Jinying Chen, Ran Xu, Heather Angier, Amy G Huebschmann, Mayuko Ito Fukunaga, Krisda H Chaiyachati, Katharine A Rendle, Kim Robien, Lisa DiMartino, Daniel J Amante, Jamie M Faro, Maura M Kepper, Alex T Ramsey, Eric Bressman, Rachel Gold","doi":"10.2196/49002","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A substantial percentage of the US population is not up to date on guideline-recommended cancer screenings. Identifying interventions that effectively improve screening rates would enhance the delivery of such screening. Interventions involving health IT (HIT) show promise, but much remains unknown about how HIT is optimized to support cancer screening in primary care.</p><p><strong>Objective: </strong>This scoping review aims to identify (1) HIT-based interventions that effectively support guideline concordance in breast, cervical, and colorectal cancer screening provision and follow-up in the primary care setting and (2) barriers or facilitators to the implementation of effective HIT in this setting.</p><p><strong>Methods: </strong>Following scoping review guidelines, we searched MEDLINE, CINAHL Plus, Web of Science, and IEEE Xplore databases for US-based studies from 2015 to 2021 that featured HIT targeting breast, colorectal, and cervical cancer screening in primary care. Studies were dual screened using a review criteria checklist. Data extraction was guided by the following implementation science frameworks: the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework; the Expert Recommendations for Implementing Change taxonomy; and implementation strategy reporting domains. It was also guided by the Integrated Technology Implementation Model that incorporates theories of both implementation science and technology adoption. Reporting was guided by PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews).</p><p><strong>Results: </strong>A total of 101 studies met the inclusion criteria. Most studies (85/101, 84.2%) involved electronic health record-based HIT interventions. The most common HIT function was clinical decision support, primarily used for panel management or at the point of care. Most studies related to HIT targeting colorectal cancer screening (83/101, 82.2%), followed by studies related to breast cancer screening (28/101, 27.7%), and cervical cancer screening (19/101, 18.8%). Improvements in cancer screening were associated with HIT-based interventions in most studies (36/54, 67% of colorectal cancer-relevant studies; 9/14, 64% of breast cancer-relevant studies; and 7/10, 70% of cervical cancer-relevant studies). Most studies (79/101, 78.2%) reported on the reach of certain interventions, while 17.8% (18/101) of the included studies reported on the adoption or maintenance. Reported barriers and facilitators to HIT adoption primarily related to inner context factors of primary care settings (eg, staffing and organizational policies that support or hinder HIT adoption). Implementation strategies for HIT adoption were reported in 23.8% (24/101) of the included studies.</p><p><strong>Conclusions: </strong>There are substantial evidence gaps regarding the effectiveness of HIT-based interventions, especially those targeting guideline-concordant breast and colorectal cancer screening in primary care. Even less is known about how to enhance the adoption of technologies that have been proven effective in supporting breast, colorectal, or cervical cancer screening. Research is needed to ensure that the potential benefits of effective HIT-based interventions equitably reach diverse primary care populations.</p>","PeriodicalId":45538,"journal":{"name":"JMIR Cancer","volume":"10 ","pages":"e49002"},"PeriodicalIF":2.7000,"publicationDate":"2024-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11094604/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementation of Health IT for Cancer Screening in US Primary Care: Scoping Review.\",\"authors\":\"Constance Owens-Jasey, Jinying Chen, Ran Xu, Heather Angier, Amy G Huebschmann, Mayuko Ito Fukunaga, Krisda H Chaiyachati, Katharine A Rendle, Kim Robien, Lisa DiMartino, Daniel J Amante, Jamie M Faro, Maura M Kepper, Alex T Ramsey, Eric Bressman, Rachel Gold\",\"doi\":\"10.2196/49002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A substantial percentage of the US population is not up to date on guideline-recommended cancer screenings. Identifying interventions that effectively improve screening rates would enhance the delivery of such screening. Interventions involving health IT (HIT) show promise, but much remains unknown about how HIT is optimized to support cancer screening in primary care.</p><p><strong>Objective: </strong>This scoping review aims to identify (1) HIT-based interventions that effectively support guideline concordance in breast, cervical, and colorectal cancer screening provision and follow-up in the primary care setting and (2) barriers or facilitators to the implementation of effective HIT in this setting.</p><p><strong>Methods: </strong>Following scoping review guidelines, we searched MEDLINE, CINAHL Plus, Web of Science, and IEEE Xplore databases for US-based studies from 2015 to 2021 that featured HIT targeting breast, colorectal, and cervical cancer screening in primary care. Studies were dual screened using a review criteria checklist. Data extraction was guided by the following implementation science frameworks: the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework; the Expert Recommendations for Implementing Change taxonomy; and implementation strategy reporting domains. It was also guided by the Integrated Technology Implementation Model that incorporates theories of both implementation science and technology adoption. Reporting was guided by PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews).</p><p><strong>Results: </strong>A total of 101 studies met the inclusion criteria. Most studies (85/101, 84.2%) involved electronic health record-based HIT interventions. The most common HIT function was clinical decision support, primarily used for panel management or at the point of care. Most studies related to HIT targeting colorectal cancer screening (83/101, 82.2%), followed by studies related to breast cancer screening (28/101, 27.7%), and cervical cancer screening (19/101, 18.8%). Improvements in cancer screening were associated with HIT-based interventions in most studies (36/54, 67% of colorectal cancer-relevant studies; 9/14, 64% of breast cancer-relevant studies; and 7/10, 70% of cervical cancer-relevant studies). Most studies (79/101, 78.2%) reported on the reach of certain interventions, while 17.8% (18/101) of the included studies reported on the adoption or maintenance. Reported barriers and facilitators to HIT adoption primarily related to inner context factors of primary care settings (eg, staffing and organizational policies that support or hinder HIT adoption). Implementation strategies for HIT adoption were reported in 23.8% (24/101) of the included studies.</p><p><strong>Conclusions: </strong>There are substantial evidence gaps regarding the effectiveness of HIT-based interventions, especially those targeting guideline-concordant breast and colorectal cancer screening in primary care. Even less is known about how to enhance the adoption of technologies that have been proven effective in supporting breast, colorectal, or cervical cancer screening. Research is needed to ensure that the potential benefits of effective HIT-based interventions equitably reach diverse primary care populations.</p>\",\"PeriodicalId\":45538,\"journal\":{\"name\":\"JMIR Cancer\",\"volume\":\"10 \",\"pages\":\"e49002\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11094604/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Cancer\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/49002\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/49002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:美国有相当大比例的人口没有接受指南推荐的最新癌症筛查。确定能够有效提高筛查率的干预措施将有助于加强此类筛查的实施。涉及医疗信息技术(HIT)的干预措施显示出了前景,但关于如何优化 HIT 以支持初级医疗中的癌症筛查,仍有许多未知之处:本范围界定综述旨在确定(1)基于 HIT 的干预措施,这些干预措施可有效支持初级医疗环境中乳腺癌、宫颈癌和结直肠癌筛查的提供和随访与指南保持一致;(2)在此环境中实施有效 HIT 的障碍或促进因素:根据范围界定综述指南,我们在 MEDLINE、CINAHL Plus、Web of Science 和 IEEE Xplore 数据库中检索了 2015 年至 2021 年期间以美国为基地的研究,这些研究以初级医疗中针对乳腺癌、结直肠癌和宫颈癌筛查的 HIT 为主题。研究采用审查标准清单进行双重筛选。数据提取以下列实施科学框架为指导:普及、效果、采用、实施和维护框架;实施变革的专家建议分类法;以及实施策略报告域。此外,还以综合技术实施模型为指导,该模型融合了实施科学和技术采用的理论。报告以 PRISMA-ScR(系统性综述和元分析的首选报告项目,范围综述的扩展)为指导:结果:共有 101 项研究符合纳入标准。大多数研究(85/101,84.2%)涉及基于电子健康记录的 HIT 干预。最常见的 HIT 功能是临床决策支持,主要用于小组管理或护理点。大多数与 HIT 相关的研究都针对大肠癌筛查(83/101,82.2%),其次是乳腺癌筛查(28/101,27.7%)和宫颈癌筛查(19/101,18.8%)。在大多数研究中,癌症筛查的改善与基于 HIT 的干预措施有关(36/54,占结直肠癌相关研究的 67%;9/14,占乳腺癌相关研究的 64%;7/10,占宫颈癌相关研究的 70%)。大多数研究(79/101,78.2%)报告了某些干预措施的覆盖范围,而纳入的研究中有 17.8%(18/101)报告了干预措施的采用或维持情况。所报告的采用 HIT 的障碍和促进因素主要与基层医疗机构的内在环境因素有关(例如,支持或阻碍采用 HIT 的人员配备和组织政策)。在纳入的研究中,23.8%(24/101)的研究报告了采用 HIT 的实施策略:结论:关于基于 HIT 的干预措施的有效性,尤其是针对初级保健中与指南一致的乳腺癌和结直肠癌筛查的干预措施的有效性,还存在很大的证据差距。至于如何促进采用已被证明能有效支持乳腺癌、结肠直肠癌或宫颈癌筛查的技术,人们所知就更少了。需要开展研究,以确保有效的基于 HIT 的干预措施的潜在益处公平地惠及不同的初级保健人群。
Implementation of Health IT for Cancer Screening in US Primary Care: Scoping Review.
Background: A substantial percentage of the US population is not up to date on guideline-recommended cancer screenings. Identifying interventions that effectively improve screening rates would enhance the delivery of such screening. Interventions involving health IT (HIT) show promise, but much remains unknown about how HIT is optimized to support cancer screening in primary care.
Objective: This scoping review aims to identify (1) HIT-based interventions that effectively support guideline concordance in breast, cervical, and colorectal cancer screening provision and follow-up in the primary care setting and (2) barriers or facilitators to the implementation of effective HIT in this setting.
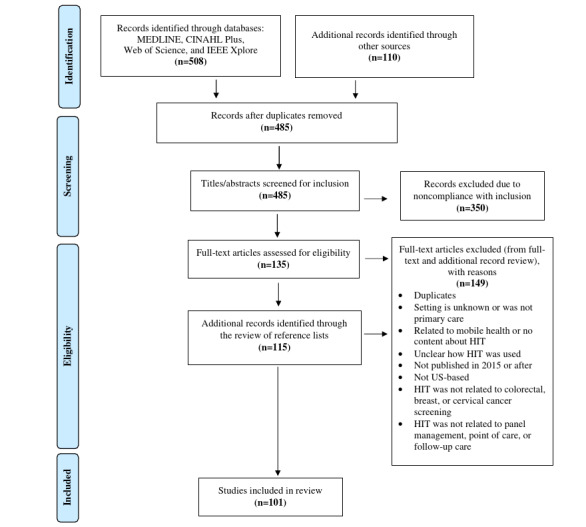
Methods: Following scoping review guidelines, we searched MEDLINE, CINAHL Plus, Web of Science, and IEEE Xplore databases for US-based studies from 2015 to 2021 that featured HIT targeting breast, colorectal, and cervical cancer screening in primary care. Studies were dual screened using a review criteria checklist. Data extraction was guided by the following implementation science frameworks: the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework; the Expert Recommendations for Implementing Change taxonomy; and implementation strategy reporting domains. It was also guided by the Integrated Technology Implementation Model that incorporates theories of both implementation science and technology adoption. Reporting was guided by PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews).
Results: A total of 101 studies met the inclusion criteria. Most studies (85/101, 84.2%) involved electronic health record-based HIT interventions. The most common HIT function was clinical decision support, primarily used for panel management or at the point of care. Most studies related to HIT targeting colorectal cancer screening (83/101, 82.2%), followed by studies related to breast cancer screening (28/101, 27.7%), and cervical cancer screening (19/101, 18.8%). Improvements in cancer screening were associated with HIT-based interventions in most studies (36/54, 67% of colorectal cancer-relevant studies; 9/14, 64% of breast cancer-relevant studies; and 7/10, 70% of cervical cancer-relevant studies). Most studies (79/101, 78.2%) reported on the reach of certain interventions, while 17.8% (18/101) of the included studies reported on the adoption or maintenance. Reported barriers and facilitators to HIT adoption primarily related to inner context factors of primary care settings (eg, staffing and organizational policies that support or hinder HIT adoption). Implementation strategies for HIT adoption were reported in 23.8% (24/101) of the included studies.
Conclusions: There are substantial evidence gaps regarding the effectiveness of HIT-based interventions, especially those targeting guideline-concordant breast and colorectal cancer screening in primary care. Even less is known about how to enhance the adoption of technologies that have been proven effective in supporting breast, colorectal, or cervical cancer screening. Research is needed to ensure that the potential benefits of effective HIT-based interventions equitably reach diverse primary care populations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


