Samira Merali, David H. Salinger, Maria Palmisano, Amy J. Sehnert, Neelima Thanneer, Hyunmoon Back, Julie D. Seroogy, Daniel D. Gretler, Amit Roy, Vidya Perera
{"title":"通过对阻塞性肥厚型心肌病成人患者进行基于模型的分析,推荐使用马伐康坦。","authors":"Samira Merali, David H. Salinger, Maria Palmisano, Amy J. Sehnert, Neelima Thanneer, Hyunmoon Back, Julie D. Seroogy, Daniel D. Gretler, Amit Roy, Vidya Perera","doi":"10.1002/psp4.13138","DOIUrl":null,"url":null,"abstract":"<p>Mavacamten is the first cardiac myosin inhibitor approved by the US Food and Drug Administration for the treatment of adults with symptomatic obstructive hypertrophic cardiomyopathy (HCM). The phase III EXPLORER-HCM (NCT03470545) study used a dose-titration scheme based on mavacamten exposure and echocardiographic assessment of Valsalva left ventricular outflow tract gradient (VLVOTg) and left ventricular ejection fraction (LVEF). Using population pharmacokinetic/exposure-response modeling and simulations of virtual patients, this in silico study evaluated alternative dose-titration regimens for mavacamten, including regimens that were guided by echocardiographic measures only. Mavacamten exposure-response models for VLVOTg (efficacy) and LVEF (safety) were developed using patient data from five clinical studies and characterized using nonlinear mixed-effects models. Simulations of five echocardiography-guided regimens were performed in virtual cohorts constructed based on either expected or equal population distributions of cytochrome P450 2C19 (CYP2C19) metabolizer phenotypes. Each regimen aimed to maximize the proportions of patients who achieved a VLVOTg below 30 mm Hg while maintaining LVEF above 50% over 40 weeks and 104 weeks, respectively. The exposure-response models successfully characterized mavacamten efficacy and safety parameters. Overall, the simulated regimen with the optimal benefit–risk profile across CYP2C19 phenotypes had steps for down-titration at weeks 4 and 8 (for VLVOTg <20 mm Hg), and up-titration at week 12 (for VLVOTg ≥30 mm Hg and LVEF ≥55%), and every 12 weeks thereafter. This simulation-optimized regimen is recommended in the mavacamten US prescribing information.</p>","PeriodicalId":10774,"journal":{"name":"CPT: Pharmacometrics & Systems Pharmacology","volume":null,"pages":null},"PeriodicalIF":3.1000,"publicationDate":"2024-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/psp4.13138","citationCount":"0","resultStr":"{\"title\":\"Recommendation of mavacamten posology by model-based analyses in adults with obstructive hypertrophic cardiomyopathy\",\"authors\":\"Samira Merali, David H. Salinger, Maria Palmisano, Amy J. Sehnert, Neelima Thanneer, Hyunmoon Back, Julie D. Seroogy, Daniel D. Gretler, Amit Roy, Vidya Perera\",\"doi\":\"10.1002/psp4.13138\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Mavacamten is the first cardiac myosin inhibitor approved by the US Food and Drug Administration for the treatment of adults with symptomatic obstructive hypertrophic cardiomyopathy (HCM). The phase III EXPLORER-HCM (NCT03470545) study used a dose-titration scheme based on mavacamten exposure and echocardiographic assessment of Valsalva left ventricular outflow tract gradient (VLVOTg) and left ventricular ejection fraction (LVEF). Using population pharmacokinetic/exposure-response modeling and simulations of virtual patients, this in silico study evaluated alternative dose-titration regimens for mavacamten, including regimens that were guided by echocardiographic measures only. Mavacamten exposure-response models for VLVOTg (efficacy) and LVEF (safety) were developed using patient data from five clinical studies and characterized using nonlinear mixed-effects models. Simulations of five echocardiography-guided regimens were performed in virtual cohorts constructed based on either expected or equal population distributions of cytochrome P450 2C19 (CYP2C19) metabolizer phenotypes. Each regimen aimed to maximize the proportions of patients who achieved a VLVOTg below 30 mm Hg while maintaining LVEF above 50% over 40 weeks and 104 weeks, respectively. The exposure-response models successfully characterized mavacamten efficacy and safety parameters. Overall, the simulated regimen with the optimal benefit–risk profile across CYP2C19 phenotypes had steps for down-titration at weeks 4 and 8 (for VLVOTg <20 mm Hg), and up-titration at week 12 (for VLVOTg ≥30 mm Hg and LVEF ≥55%), and every 12 weeks thereafter. This simulation-optimized regimen is recommended in the mavacamten US prescribing information.</p>\",\"PeriodicalId\":10774,\"journal\":{\"name\":\"CPT: Pharmacometrics & Systems Pharmacology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/psp4.13138\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CPT: Pharmacometrics & Systems Pharmacology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/psp4.13138\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CPT: Pharmacometrics & Systems Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/psp4.13138","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Recommendation of mavacamten posology by model-based analyses in adults with obstructive hypertrophic cardiomyopathy
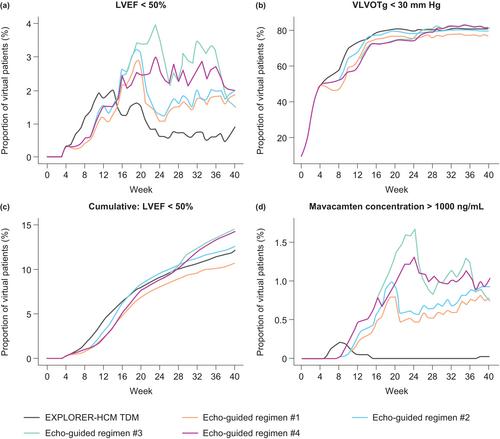
Mavacamten is the first cardiac myosin inhibitor approved by the US Food and Drug Administration for the treatment of adults with symptomatic obstructive hypertrophic cardiomyopathy (HCM). The phase III EXPLORER-HCM (NCT03470545) study used a dose-titration scheme based on mavacamten exposure and echocardiographic assessment of Valsalva left ventricular outflow tract gradient (VLVOTg) and left ventricular ejection fraction (LVEF). Using population pharmacokinetic/exposure-response modeling and simulations of virtual patients, this in silico study evaluated alternative dose-titration regimens for mavacamten, including regimens that were guided by echocardiographic measures only. Mavacamten exposure-response models for VLVOTg (efficacy) and LVEF (safety) were developed using patient data from five clinical studies and characterized using nonlinear mixed-effects models. Simulations of five echocardiography-guided regimens were performed in virtual cohorts constructed based on either expected or equal population distributions of cytochrome P450 2C19 (CYP2C19) metabolizer phenotypes. Each regimen aimed to maximize the proportions of patients who achieved a VLVOTg below 30 mm Hg while maintaining LVEF above 50% over 40 weeks and 104 weeks, respectively. The exposure-response models successfully characterized mavacamten efficacy and safety parameters. Overall, the simulated regimen with the optimal benefit–risk profile across CYP2C19 phenotypes had steps for down-titration at weeks 4 and 8 (for VLVOTg <20 mm Hg), and up-titration at week 12 (for VLVOTg ≥30 mm Hg and LVEF ≥55%), and every 12 weeks thereafter. This simulation-optimized regimen is recommended in the mavacamten US prescribing information.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


