{"title":"高分子量肾上腺皮质激素分泌型亚临床库欣病","authors":"Takahiko Inukai, Nozomi Harai, Yukie Nakagawa, Tadatsugu Hosokawa, Airi Antoku, Yuko Muroi, Masakazu Ogiwara, Kyoichiro Tsuchiya","doi":"10.1155/2024/8721614","DOIUrl":null,"url":null,"abstract":"<p><p>Production of the high-molecular-weight forms of adrenocorticotropic hormone (big-ACTH) has been reported in a small number of ectopic ACTH syndrome and ACTH-producing pituitary macroadenoma. However, perioperative changes in big-ACTH in patients with subclinical Cushing's disease have not been reported. A 63-year-old woman presented 25 × 20 × 20-mm-sized macroadenoma in the pituitary gland. Her early morning plasma ACTH and cortisol levels were 111 pg/mL and 11.6 <i>μ</i>g/dL, respectively. Cushingoid features and diurnal variation in plasma cortisol levels were not observed. The patient's urinary free cortisol (UFC) was 59.3 <i>μ</i>g/day. The corticotropin-releasing hormone (CRH) test showed that plasma ACTH levels were 1.5 times higher than the preload value. The overnight dexamethasone suppression test (DST) showed that the plasma cortisol level was not suppressed by 0.5 mg of dexamethasone (DEX) but was suppressed by 8 mg of DEX. Inferior pyramidal sinus sampling was consistent with Cushing's disease. Taken together, the patient was clinically diagnosed with subclinical Cushing's disease caused by an ACTH-producing pituitary adenoma. Endoscopic transsphenoidal adenomectomy was performed. In the postoperative CRH test, plasma ACTH levels showed six-fold increase. The postoperative DST showed cortisol suppression at 0.5 mg of DEX. The UFC levels decreased to 35.1 <i>μ</i>g/day. Pituitary contrast-enhanced MRI revealed no residual tumor, and plasma ACTH and cortisol levels remained within normal ranges. Gel filtration of preoperative and postoperative plasma ACTH was performed, and a high molecular weight fraction of ACTH was detected, which markedly decreased postoperatively. The absence of Cushingoid features and the lack of significant cortisol hypersecretion in this case were thought to be due in part to big-ACTH, which has low bioactivity. By careful evaluation of laboratory and clinical findings, we identified it as a big-ACTH-producing adenoma. This is the first report of a case in which the big-ACTH transition was observed perioperative and is a valuable case.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2024 ","pages":"8721614"},"PeriodicalIF":0.9000,"publicationDate":"2024-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10985640/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subclinical Cushing's Disease with High-Molecular-Weight Forms of Adrenocorticotropic Hormone Production.\",\"authors\":\"Takahiko Inukai, Nozomi Harai, Yukie Nakagawa, Tadatsugu Hosokawa, Airi Antoku, Yuko Muroi, Masakazu Ogiwara, Kyoichiro Tsuchiya\",\"doi\":\"10.1155/2024/8721614\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Production of the high-molecular-weight forms of adrenocorticotropic hormone (big-ACTH) has been reported in a small number of ectopic ACTH syndrome and ACTH-producing pituitary macroadenoma. However, perioperative changes in big-ACTH in patients with subclinical Cushing's disease have not been reported. A 63-year-old woman presented 25 × 20 × 20-mm-sized macroadenoma in the pituitary gland. Her early morning plasma ACTH and cortisol levels were 111 pg/mL and 11.6 <i>μ</i>g/dL, respectively. Cushingoid features and diurnal variation in plasma cortisol levels were not observed. The patient's urinary free cortisol (UFC) was 59.3 <i>μ</i>g/day. The corticotropin-releasing hormone (CRH) test showed that plasma ACTH levels were 1.5 times higher than the preload value. The overnight dexamethasone suppression test (DST) showed that the plasma cortisol level was not suppressed by 0.5 mg of dexamethasone (DEX) but was suppressed by 8 mg of DEX. Inferior pyramidal sinus sampling was consistent with Cushing's disease. Taken together, the patient was clinically diagnosed with subclinical Cushing's disease caused by an ACTH-producing pituitary adenoma. Endoscopic transsphenoidal adenomectomy was performed. In the postoperative CRH test, plasma ACTH levels showed six-fold increase. The postoperative DST showed cortisol suppression at 0.5 mg of DEX. The UFC levels decreased to 35.1 <i>μ</i>g/day. Pituitary contrast-enhanced MRI revealed no residual tumor, and plasma ACTH and cortisol levels remained within normal ranges. Gel filtration of preoperative and postoperative plasma ACTH was performed, and a high molecular weight fraction of ACTH was detected, which markedly decreased postoperatively. The absence of Cushingoid features and the lack of significant cortisol hypersecretion in this case were thought to be due in part to big-ACTH, which has low bioactivity. By careful evaluation of laboratory and clinical findings, we identified it as a big-ACTH-producing adenoma. This is the first report of a case in which the big-ACTH transition was observed perioperative and is a valuable case.</p>\",\"PeriodicalId\":9621,\"journal\":{\"name\":\"Case Reports in Endocrinology\",\"volume\":\"2024 \",\"pages\":\"8721614\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-03-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10985640/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/8721614\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/8721614","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Subclinical Cushing's Disease with High-Molecular-Weight Forms of Adrenocorticotropic Hormone Production.
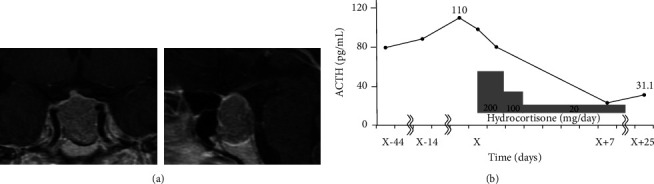
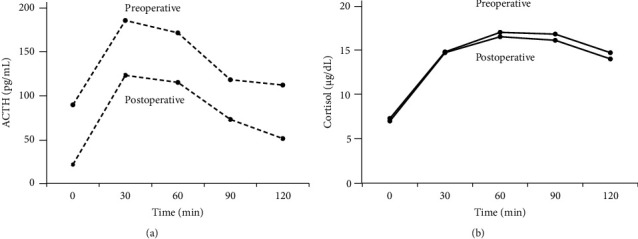
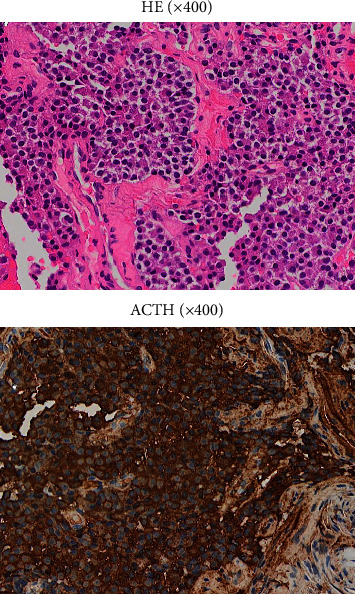
Production of the high-molecular-weight forms of adrenocorticotropic hormone (big-ACTH) has been reported in a small number of ectopic ACTH syndrome and ACTH-producing pituitary macroadenoma. However, perioperative changes in big-ACTH in patients with subclinical Cushing's disease have not been reported. A 63-year-old woman presented 25 × 20 × 20-mm-sized macroadenoma in the pituitary gland. Her early morning plasma ACTH and cortisol levels were 111 pg/mL and 11.6 μg/dL, respectively. Cushingoid features and diurnal variation in plasma cortisol levels were not observed. The patient's urinary free cortisol (UFC) was 59.3 μg/day. The corticotropin-releasing hormone (CRH) test showed that plasma ACTH levels were 1.5 times higher than the preload value. The overnight dexamethasone suppression test (DST) showed that the plasma cortisol level was not suppressed by 0.5 mg of dexamethasone (DEX) but was suppressed by 8 mg of DEX. Inferior pyramidal sinus sampling was consistent with Cushing's disease. Taken together, the patient was clinically diagnosed with subclinical Cushing's disease caused by an ACTH-producing pituitary adenoma. Endoscopic transsphenoidal adenomectomy was performed. In the postoperative CRH test, plasma ACTH levels showed six-fold increase. The postoperative DST showed cortisol suppression at 0.5 mg of DEX. The UFC levels decreased to 35.1 μg/day. Pituitary contrast-enhanced MRI revealed no residual tumor, and plasma ACTH and cortisol levels remained within normal ranges. Gel filtration of preoperative and postoperative plasma ACTH was performed, and a high molecular weight fraction of ACTH was detected, which markedly decreased postoperatively. The absence of Cushingoid features and the lack of significant cortisol hypersecretion in this case were thought to be due in part to big-ACTH, which has low bioactivity. By careful evaluation of laboratory and clinical findings, we identified it as a big-ACTH-producing adenoma. This is the first report of a case in which the big-ACTH transition was observed perioperative and is a valuable case.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


