Mathias Orellana-Donoso, Diego Romero-Zucchino, Alonso Fuentes-Abarca, Priscila Aravena-Ríos, Juan Sanchis-Gimeno, Marko Konschake, Pablo Nova-Baeza, Juan José Valenzuela-Fuenzalida
{"title":"眶下管变异及其临床和手术影响。系统回顾","authors":"Mathias Orellana-Donoso, Diego Romero-Zucchino, Alonso Fuentes-Abarca, Priscila Aravena-Ríos, Juan Sanchis-Gimeno, Marko Konschake, Pablo Nova-Baeza, Juan José Valenzuela-Fuenzalida","doi":"10.1007/s00276-024-03348-3","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>Recent literature highlights anomalous cranial nerves in the sinonasal region, notably in the sphenoid and maxillary sinuses, linked to anatomical factors. However, data on the suspended infraorbital canal (IOC) variant is scarce in cross-sectional imaging. Anatomical variations in the sphenoid sinuses, including optic, maxillary, and vidian nerves, raise interest among specialists involved in advanced sinonasal procedures. The infraorbital nerve’s (ION) course along the orbital floor and its abnormal positioning within the orbital and maxillary sinus region pose risks of iatrogenic complications. A comprehensive radiological assessment is crucial before sinonasal surgeries. Cone-beam computed tomography (CBCT) is preferred for its spatial resolution and reduced radiation exposure.</p><h3 data-test=\"abstract-sub-heading\">Objective</h3><p>The aim of this study was to describe the prevalence of anatomical variants of the infraorbital canal (IOC) and report its association with clinical condition or surgical implication.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>We searched Medline, Scopus, Web of Science, Google Scholar, CINAHL, and LILACS databases from their inception up to June 2023. Two authors independently performed the search, study selection, data extraction, and assessed the methodological quality with assurance tool for anatomical studies (AQUA). Finally, the pooled prevalence was estimated using a random effects model.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Preliminary results show that three types are prevalent, type 1: the IOC does not bulge into the maxillary sinus (MS); therefore, the infraorbital foramen through the anterior wall of MS could be used for identification of the ION. Type 2: the IOC divided the orbital floor into medial and lateral aspects. Type 3: the IOC hangs in the MS and the entire orbital floor lying above the IOC. From which the clinical implications where mainly surgical, in type 1 the infraorbital foramen through the anterior wall of MS could be used for identification of the ION, while in type 2, since the lateral orbital floor could not be directly accessed an inferiorly transposition of ION is helpful to expose the lateral orbital wall directly with a 0 scope; or using angled endoscopes and instruments, however, the authors opinion is that direct exposure potentially facilitates the visualization and management in complex situations such as residual or recurrent mass, foreign body, and fracture located at the lateral aspect of the canal. Lastly, in type 3, the ION it’s easily exposed with a 0° scope.</p><h3 data-test=\"abstract-sub-heading\">Conclusions</h3><p>This systematic review identified four IOC variants: Type 1, within or below the MS roof; Type 2, partially protruding into the sinus; Type 3, fully protruding into the sinus or suspended from the roof; and Type 4, in the orbital floor. Clinical recommendations aim to prevent nerve injuries and enhance preoperative assessments. However, the lack of consistent statistical methods limits robust associations between IOC variants and clinical outcomes. Data heterogeneity and the absence of standardized reporting impede meta-analysis. Future research should prioritize detailed reporting, objective measurements, and statistical approaches for a comprehensive understanding of IOC variants and their clinical implications.</p><p>Open Science Framework (OSF): https://doi.org/10.17605/OSF.IO/UGYFZ.</p>","PeriodicalId":49296,"journal":{"name":"Surgical and Radiologic Anatomy","volume":"2012 1","pages":""},"PeriodicalIF":1.2000,"publicationDate":"2024-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Infraorbital canal variants and its clinical and surgical implications. A systematic review\",\"authors\":\"Mathias Orellana-Donoso, Diego Romero-Zucchino, Alonso Fuentes-Abarca, Priscila Aravena-Ríos, Juan Sanchis-Gimeno, Marko Konschake, Pablo Nova-Baeza, Juan José Valenzuela-Fuenzalida\",\"doi\":\"10.1007/s00276-024-03348-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Background</h3><p>Recent literature highlights anomalous cranial nerves in the sinonasal region, notably in the sphenoid and maxillary sinuses, linked to anatomical factors. However, data on the suspended infraorbital canal (IOC) variant is scarce in cross-sectional imaging. Anatomical variations in the sphenoid sinuses, including optic, maxillary, and vidian nerves, raise interest among specialists involved in advanced sinonasal procedures. The infraorbital nerve’s (ION) course along the orbital floor and its abnormal positioning within the orbital and maxillary sinus region pose risks of iatrogenic complications. A comprehensive radiological assessment is crucial before sinonasal surgeries. Cone-beam computed tomography (CBCT) is preferred for its spatial resolution and reduced radiation exposure.</p><h3 data-test=\\\"abstract-sub-heading\\\">Objective</h3><p>The aim of this study was to describe the prevalence of anatomical variants of the infraorbital canal (IOC) and report its association with clinical condition or surgical implication.</p><h3 data-test=\\\"abstract-sub-heading\\\">Methods</h3><p>We searched Medline, Scopus, Web of Science, Google Scholar, CINAHL, and LILACS databases from their inception up to June 2023. Two authors independently performed the search, study selection, data extraction, and assessed the methodological quality with assurance tool for anatomical studies (AQUA). Finally, the pooled prevalence was estimated using a random effects model.</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>Preliminary results show that three types are prevalent, type 1: the IOC does not bulge into the maxillary sinus (MS); therefore, the infraorbital foramen through the anterior wall of MS could be used for identification of the ION. Type 2: the IOC divided the orbital floor into medial and lateral aspects. Type 3: the IOC hangs in the MS and the entire orbital floor lying above the IOC. From which the clinical implications where mainly surgical, in type 1 the infraorbital foramen through the anterior wall of MS could be used for identification of the ION, while in type 2, since the lateral orbital floor could not be directly accessed an inferiorly transposition of ION is helpful to expose the lateral orbital wall directly with a 0 scope; or using angled endoscopes and instruments, however, the authors opinion is that direct exposure potentially facilitates the visualization and management in complex situations such as residual or recurrent mass, foreign body, and fracture located at the lateral aspect of the canal. Lastly, in type 3, the ION it’s easily exposed with a 0° scope.</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusions</h3><p>This systematic review identified four IOC variants: Type 1, within or below the MS roof; Type 2, partially protruding into the sinus; Type 3, fully protruding into the sinus or suspended from the roof; and Type 4, in the orbital floor. Clinical recommendations aim to prevent nerve injuries and enhance preoperative assessments. However, the lack of consistent statistical methods limits robust associations between IOC variants and clinical outcomes. Data heterogeneity and the absence of standardized reporting impede meta-analysis. Future research should prioritize detailed reporting, objective measurements, and statistical approaches for a comprehensive understanding of IOC variants and their clinical implications.</p><p>Open Science Framework (OSF): https://doi.org/10.17605/OSF.IO/UGYFZ.</p>\",\"PeriodicalId\":49296,\"journal\":{\"name\":\"Surgical and Radiologic Anatomy\",\"volume\":\"2012 1\",\"pages\":\"\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-04-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical and Radiologic Anatomy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00276-024-03348-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ANATOMY & MORPHOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical and Radiologic Anatomy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00276-024-03348-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANATOMY & MORPHOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景最近的文献强调了鼻窦区域的颅神经异常,特别是蝶窦和上颌窦,这与解剖因素有关。然而,横断面成像中有关悬吊眶下管(IOC)变异的数据却很少。蝶窦的解剖变异,包括视神经、上颌神经和吠陀神经,引起了从事高级鼻窦手术的专家的兴趣。眶下神经(ION)沿着眶底的走向及其在眶窦和上颌窦区域内的异常位置会带来先天性并发症的风险。在进行鼻窦手术之前,全面的放射学评估至关重要。本研究旨在描述眶下管(IOC)解剖变异的发生率,并报告其与临床状况或手术影响的关系。方法我们检索了 Medline、Scopus、Web of Science、Google Scholar、CINAHL 和 LILACS 数据库从开始到 2023 年 6 月的所有内容。两位作者独立完成了检索、研究选择、数据提取,并使用解剖学研究保证工具(AQUA)评估了方法学质量。最后,使用随机效应模型估算了汇总的患病率。结果初步结果显示,有三种类型比较流行:类型1:IOC没有凸入上颌窦(MS);因此,可以使用穿过MS前壁的眶下孔来识别ION。类型 2:IOC 将眶底分为内侧和外侧。类型 3:IOC 悬挂在 MS 中,整个眶底位于 IOC 的上方。在第1型中,通过MS前壁的眶下孔可用于识别ION,而在第2型中,由于无法直接进入外侧眶底,因此将ION向下转位有助于用0号镜直接暴露外侧眶壁;然而,作者认为,直接暴露可能有助于观察和处理复杂情况,如位于眶管外侧的残留或复发性肿块、异物和骨折。最后,在类型 3 中,ION 很容易用 0° 镜暴露:本系统综述确定了四种 IOC 变体:第 1 型,位于 MS 屋顶内或低于 MS 屋顶;第 2 型,部分突出于窦内;第 3 型,完全突出于窦内或悬挂于窦顶;第 4 型,位于眶底。临床建议旨在防止神经损伤并加强术前评估。然而,由于缺乏一致的统计方法,限制了 IOC 变体与临床结果之间的紧密联系。数据异质性和标准化报告的缺乏阻碍了荟萃分析。未来的研究应优先考虑详细报告、客观测量和统计方法,以全面了解IOC变异及其临床影响。开放科学框架(OSF):https://doi.org/10.17605/OSF.IO/UGYFZ。
Infraorbital canal variants and its clinical and surgical implications. A systematic review
Background
Recent literature highlights anomalous cranial nerves in the sinonasal region, notably in the sphenoid and maxillary sinuses, linked to anatomical factors. However, data on the suspended infraorbital canal (IOC) variant is scarce in cross-sectional imaging. Anatomical variations in the sphenoid sinuses, including optic, maxillary, and vidian nerves, raise interest among specialists involved in advanced sinonasal procedures. The infraorbital nerve’s (ION) course along the orbital floor and its abnormal positioning within the orbital and maxillary sinus region pose risks of iatrogenic complications. A comprehensive radiological assessment is crucial before sinonasal surgeries. Cone-beam computed tomography (CBCT) is preferred for its spatial resolution and reduced radiation exposure.
Objective
The aim of this study was to describe the prevalence of anatomical variants of the infraorbital canal (IOC) and report its association with clinical condition or surgical implication.
Methods
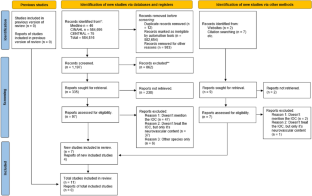
We searched Medline, Scopus, Web of Science, Google Scholar, CINAHL, and LILACS databases from their inception up to June 2023. Two authors independently performed the search, study selection, data extraction, and assessed the methodological quality with assurance tool for anatomical studies (AQUA). Finally, the pooled prevalence was estimated using a random effects model.
Results
Preliminary results show that three types are prevalent, type 1: the IOC does not bulge into the maxillary sinus (MS); therefore, the infraorbital foramen through the anterior wall of MS could be used for identification of the ION. Type 2: the IOC divided the orbital floor into medial and lateral aspects. Type 3: the IOC hangs in the MS and the entire orbital floor lying above the IOC. From which the clinical implications where mainly surgical, in type 1 the infraorbital foramen through the anterior wall of MS could be used for identification of the ION, while in type 2, since the lateral orbital floor could not be directly accessed an inferiorly transposition of ION is helpful to expose the lateral orbital wall directly with a 0 scope; or using angled endoscopes and instruments, however, the authors opinion is that direct exposure potentially facilitates the visualization and management in complex situations such as residual or recurrent mass, foreign body, and fracture located at the lateral aspect of the canal. Lastly, in type 3, the ION it’s easily exposed with a 0° scope.
Conclusions
This systematic review identified four IOC variants: Type 1, within or below the MS roof; Type 2, partially protruding into the sinus; Type 3, fully protruding into the sinus or suspended from the roof; and Type 4, in the orbital floor. Clinical recommendations aim to prevent nerve injuries and enhance preoperative assessments. However, the lack of consistent statistical methods limits robust associations between IOC variants and clinical outcomes. Data heterogeneity and the absence of standardized reporting impede meta-analysis. Future research should prioritize detailed reporting, objective measurements, and statistical approaches for a comprehensive understanding of IOC variants and their clinical implications.
Open Science Framework (OSF): https://doi.org/10.17605/OSF.IO/UGYFZ.
期刊介绍:
Anatomy is a morphological science which cannot fail to interest the clinician. The practical application of anatomical research to clinical problems necessitates special adaptation and selectivity in choosing from numerous international works. Although there is a tendency to believe that meaningful advances in anatomy are unlikely, constant revision is necessary. Surgical and Radiologic Anatomy, the first international journal of Clinical anatomy has been created in this spirit.
Its goal is to serve clinicians, regardless of speciality-physicians, surgeons, radiologists or other specialists-as an indispensable aid with which they can improve their knowledge of anatomy. Each issue includes: Original papers, review articles, articles on the anatomical bases of medical, surgical and radiological techniques, articles of normal radiologic anatomy, brief reviews of anatomical publications of clinical interest.
Particular attention is given to high quality illustrations, which are indispensable for a better understanding of anatomical problems.
Surgical and Radiologic Anatomy is a journal written by anatomists for clinicians with a special interest in anatomy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


