Rezan Şerefoğlu, Havva Kocayiğit, Onur Palabıyık, Ayça Taş Tuna
{"title":"最小流量麻醉中自动控制和手动控制方法的比较","authors":"Rezan Şerefoğlu, Havva Kocayiğit, Onur Palabıyık, Ayça Taş Tuna","doi":"10.1007/s10877-024-01163-0","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Purpose</h3><p>New-generation anesthesia machines administer inhalation anesthetics and automatically control the fresh gas flow (FGF) rate. This study compared the administration of minimal flow anesthesia (MFA) using the automatically controlled anesthesia (ACA) module of the Mindray A9 (Shenzhen, China) anesthesia machine versus manual control by an anesthesiologist.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>We randomly divided 76 patients undergoing gynecological surgery into an ACA group (Group ACA) and a manually controlled anesthesia group (Group MCA). In Group MCA, induction was performed with a mixture of 40–60% O<sub>2</sub> and air with a 4 L/min FGF until the minimum alveolar concentration (MAC) reached 1. Next, MFA was initiated with 0.5 L/min FGF. The target fraction of inspired oxygen (FiO<sub>2</sub>) value was 35–40%. In Group ACA, the MAC was defined as 1, and the FiO<sub>2</sub> was adjusted to 35%. Depth of anesthesia, anesthetic agent (AA) consumption, time to achieve target end-tidal AA concentration, awakening times, and number of ventilator adjustments were analyzed.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>The two groups showed no statistically significant differences in depth of anesthesia or AA consumption (Group ACA: 19.1 ± 4.9 ml; Group MCA: 17.2 ± 4.5; p-value = 0.076). The ACA mode achieved the MAC target of 1 significantly faster (Group ACA: 218 ± 51 s; Group MCA: 314 ± 169 s). The number of vaporizer adjustments was 15 in the ACA group and 217 in the MCA group.</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>The ACA mode was more advantageous than the MCA mode, reaching target AA concentrations faster and requiring fewer adjustments to achieve a constant depth of anesthesia.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":null,"pages":null},"PeriodicalIF":2.0000,"publicationDate":"2024-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Comparison of automated and manual control methods in minimal flow anesthesia\",\"authors\":\"Rezan Şerefoğlu, Havva Kocayiğit, Onur Palabıyık, Ayça Taş Tuna\",\"doi\":\"10.1007/s10877-024-01163-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Purpose</h3><p>New-generation anesthesia machines administer inhalation anesthetics and automatically control the fresh gas flow (FGF) rate. This study compared the administration of minimal flow anesthesia (MFA) using the automatically controlled anesthesia (ACA) module of the Mindray A9 (Shenzhen, China) anesthesia machine versus manual control by an anesthesiologist.</p><h3 data-test=\\\"abstract-sub-heading\\\">Methods</h3><p>We randomly divided 76 patients undergoing gynecological surgery into an ACA group (Group ACA) and a manually controlled anesthesia group (Group MCA). In Group MCA, induction was performed with a mixture of 40–60% O<sub>2</sub> and air with a 4 L/min FGF until the minimum alveolar concentration (MAC) reached 1. Next, MFA was initiated with 0.5 L/min FGF. The target fraction of inspired oxygen (FiO<sub>2</sub>) value was 35–40%. In Group ACA, the MAC was defined as 1, and the FiO<sub>2</sub> was adjusted to 35%. Depth of anesthesia, anesthetic agent (AA) consumption, time to achieve target end-tidal AA concentration, awakening times, and number of ventilator adjustments were analyzed.</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>The two groups showed no statistically significant differences in depth of anesthesia or AA consumption (Group ACA: 19.1 ± 4.9 ml; Group MCA: 17.2 ± 4.5; p-value = 0.076). The ACA mode achieved the MAC target of 1 significantly faster (Group ACA: 218 ± 51 s; Group MCA: 314 ± 169 s). The number of vaporizer adjustments was 15 in the ACA group and 217 in the MCA group.</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusion</h3><p>The ACA mode was more advantageous than the MCA mode, reaching target AA concentrations faster and requiring fewer adjustments to achieve a constant depth of anesthesia.</p>\",\"PeriodicalId\":15513,\"journal\":{\"name\":\"Journal of Clinical Monitoring and Computing\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Monitoring and Computing\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10877-024-01163-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01163-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Comparison of automated and manual control methods in minimal flow anesthesia
Purpose
New-generation anesthesia machines administer inhalation anesthetics and automatically control the fresh gas flow (FGF) rate. This study compared the administration of minimal flow anesthesia (MFA) using the automatically controlled anesthesia (ACA) module of the Mindray A9 (Shenzhen, China) anesthesia machine versus manual control by an anesthesiologist.
Methods
We randomly divided 76 patients undergoing gynecological surgery into an ACA group (Group ACA) and a manually controlled anesthesia group (Group MCA). In Group MCA, induction was performed with a mixture of 40–60% O2 and air with a 4 L/min FGF until the minimum alveolar concentration (MAC) reached 1. Next, MFA was initiated with 0.5 L/min FGF. The target fraction of inspired oxygen (FiO2) value was 35–40%. In Group ACA, the MAC was defined as 1, and the FiO2 was adjusted to 35%. Depth of anesthesia, anesthetic agent (AA) consumption, time to achieve target end-tidal AA concentration, awakening times, and number of ventilator adjustments were analyzed.
Results
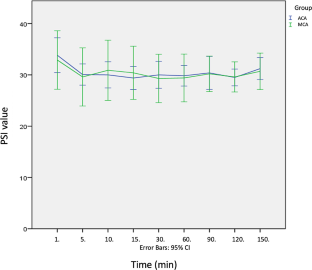
The two groups showed no statistically significant differences in depth of anesthesia or AA consumption (Group ACA: 19.1 ± 4.9 ml; Group MCA: 17.2 ± 4.5; p-value = 0.076). The ACA mode achieved the MAC target of 1 significantly faster (Group ACA: 218 ± 51 s; Group MCA: 314 ± 169 s). The number of vaporizer adjustments was 15 in the ACA group and 217 in the MCA group.
Conclusion
The ACA mode was more advantageous than the MCA mode, reaching target AA concentrations faster and requiring fewer adjustments to achieve a constant depth of anesthesia.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


