Khushboo Teotia , Yueran Jia , Naira Link Woite , Leo Anthony Celi , João Matos , Tristan Struja
{"title":"监测中的差异:以重症监护室的血糖测量为例研究如何避免虚假相关性","authors":"Khushboo Teotia , Yueran Jia , Naira Link Woite , Leo Anthony Celi , João Matos , Tristan Struja","doi":"10.1016/j.jbi.2024.104643","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>Health inequities can be influenced by demographic factors such as race and ethnicity, proficiency in English, and biological sex. Disparities may manifest as differential likelihood of testing which correlates directly with the likelihood of an intervention to address an abnormal finding. Our retrospective observational study evaluated the presence of variation in glucose measurements in the Intensive Care Unit (ICU).</p></div><div><h3>Methods</h3><p>Using the MIMIC-IV database (2008–2019), a single-center, academic referral hospital in Boston (USA), we identified adult patients meeting sepsis-3 criteria. Exclusion criteria were diabetic ketoacidosis, ICU length of stay under 1 day, and unknown race or ethnicity. We performed a logistic regression analysis to assess differential likelihoods of glucose measurements on day 1. A negative binomial regression was fitted to assess the frequency of subsequent glucose readings. Analyses were adjusted for relevant clinical confounders, and performed across three disparity proxy axes: race and ethnicity, sex, and English proficiency.</p></div><div><h3>Results</h3><p>We studied 24,927 patients, of which 19.5% represented racial and ethnic minority groups, 42.4% were female, and 9.8% had limited English proficiency. No significant differences were found for glucose measurement on day 1 in the ICU. This pattern was consistent irrespective of the axis of analysis, i.e. race and ethnicity, sex, or English proficiency. Conversely, subsequent measurement frequency revealed potential disparities. Specifically, males (incidence rate ratio (IRR) 1.06, 95% confidence interval (CI) 1.01 – 1.21), patients who identify themselves as Hispanic (IRR 1.11, 95% CI 1.01 – 1.21), or Black (IRR 1.06, 95% CI 1.01 – 1.12), and patients being English proficient (IRR 1.08, 95% CI 1.01 – 1.15) had higher chances of subsequent glucose readings.</p></div><div><h3>Conclusion</h3><p>We found disparities in ICU glucose measurements among patients with sepsis, albeit the magnitude was small. Variation in disease monitoring is a source of data bias that may lead to spurious correlations when modeling health data.</p></div>","PeriodicalId":15263,"journal":{"name":"Journal of Biomedical Informatics","volume":null,"pages":null},"PeriodicalIF":4.0000,"publicationDate":"2024-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Variation in monitoring: Glucose measurement in the ICU as a case study to preempt spurious correlations\",\"authors\":\"Khushboo Teotia , Yueran Jia , Naira Link Woite , Leo Anthony Celi , João Matos , Tristan Struja\",\"doi\":\"10.1016/j.jbi.2024.104643\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>Health inequities can be influenced by demographic factors such as race and ethnicity, proficiency in English, and biological sex. Disparities may manifest as differential likelihood of testing which correlates directly with the likelihood of an intervention to address an abnormal finding. Our retrospective observational study evaluated the presence of variation in glucose measurements in the Intensive Care Unit (ICU).</p></div><div><h3>Methods</h3><p>Using the MIMIC-IV database (2008–2019), a single-center, academic referral hospital in Boston (USA), we identified adult patients meeting sepsis-3 criteria. Exclusion criteria were diabetic ketoacidosis, ICU length of stay under 1 day, and unknown race or ethnicity. We performed a logistic regression analysis to assess differential likelihoods of glucose measurements on day 1. A negative binomial regression was fitted to assess the frequency of subsequent glucose readings. Analyses were adjusted for relevant clinical confounders, and performed across three disparity proxy axes: race and ethnicity, sex, and English proficiency.</p></div><div><h3>Results</h3><p>We studied 24,927 patients, of which 19.5% represented racial and ethnic minority groups, 42.4% were female, and 9.8% had limited English proficiency. No significant differences were found for glucose measurement on day 1 in the ICU. This pattern was consistent irrespective of the axis of analysis, i.e. race and ethnicity, sex, or English proficiency. Conversely, subsequent measurement frequency revealed potential disparities. Specifically, males (incidence rate ratio (IRR) 1.06, 95% confidence interval (CI) 1.01 – 1.21), patients who identify themselves as Hispanic (IRR 1.11, 95% CI 1.01 – 1.21), or Black (IRR 1.06, 95% CI 1.01 – 1.12), and patients being English proficient (IRR 1.08, 95% CI 1.01 – 1.15) had higher chances of subsequent glucose readings.</p></div><div><h3>Conclusion</h3><p>We found disparities in ICU glucose measurements among patients with sepsis, albeit the magnitude was small. Variation in disease monitoring is a source of data bias that may lead to spurious correlations when modeling health data.</p></div>\",\"PeriodicalId\":15263,\"journal\":{\"name\":\"Journal of Biomedical Informatics\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2024-04-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Biomedical Informatics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1532046424000613\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"COMPUTER SCIENCE, INTERDISCIPLINARY APPLICATIONS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Biomedical Informatics","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1532046424000613","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"COMPUTER SCIENCE, INTERDISCIPLINARY APPLICATIONS","Score":null,"Total":0}
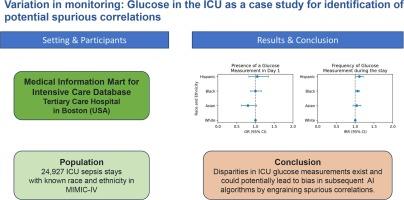
Variation in monitoring: Glucose measurement in the ICU as a case study to preempt spurious correlations
Objective
Health inequities can be influenced by demographic factors such as race and ethnicity, proficiency in English, and biological sex. Disparities may manifest as differential likelihood of testing which correlates directly with the likelihood of an intervention to address an abnormal finding. Our retrospective observational study evaluated the presence of variation in glucose measurements in the Intensive Care Unit (ICU).
Methods
Using the MIMIC-IV database (2008–2019), a single-center, academic referral hospital in Boston (USA), we identified adult patients meeting sepsis-3 criteria. Exclusion criteria were diabetic ketoacidosis, ICU length of stay under 1 day, and unknown race or ethnicity. We performed a logistic regression analysis to assess differential likelihoods of glucose measurements on day 1. A negative binomial regression was fitted to assess the frequency of subsequent glucose readings. Analyses were adjusted for relevant clinical confounders, and performed across three disparity proxy axes: race and ethnicity, sex, and English proficiency.
Results
We studied 24,927 patients, of which 19.5% represented racial and ethnic minority groups, 42.4% were female, and 9.8% had limited English proficiency. No significant differences were found for glucose measurement on day 1 in the ICU. This pattern was consistent irrespective of the axis of analysis, i.e. race and ethnicity, sex, or English proficiency. Conversely, subsequent measurement frequency revealed potential disparities. Specifically, males (incidence rate ratio (IRR) 1.06, 95% confidence interval (CI) 1.01 – 1.21), patients who identify themselves as Hispanic (IRR 1.11, 95% CI 1.01 – 1.21), or Black (IRR 1.06, 95% CI 1.01 – 1.12), and patients being English proficient (IRR 1.08, 95% CI 1.01 – 1.15) had higher chances of subsequent glucose readings.
Conclusion
We found disparities in ICU glucose measurements among patients with sepsis, albeit the magnitude was small. Variation in disease monitoring is a source of data bias that may lead to spurious correlations when modeling health data.
期刊介绍:
The Journal of Biomedical Informatics reflects a commitment to high-quality original research papers, reviews, and commentaries in the area of biomedical informatics methodology. Although we publish articles motivated by applications in the biomedical sciences (for example, clinical medicine, health care, population health, and translational bioinformatics), the journal emphasizes reports of new methodologies and techniques that have general applicability and that form the basis for the evolving science of biomedical informatics. Articles on medical devices; evaluations of implemented systems (including clinical trials of information technologies); or papers that provide insight into a biological process, a specific disease, or treatment options would generally be more suitable for publication in other venues. Papers on applications of signal processing and image analysis are often more suitable for biomedical engineering journals or other informatics journals, although we do publish papers that emphasize the information management and knowledge representation/modeling issues that arise in the storage and use of biological signals and images. System descriptions are welcome if they illustrate and substantiate the underlying methodology that is the principal focus of the report and an effort is made to address the generalizability and/or range of application of that methodology. Note also that, given the international nature of JBI, papers that deal with specific languages other than English, or with country-specific health systems or approaches, are acceptable for JBI only if they offer generalizable lessons that are relevant to the broad JBI readership, regardless of their country, language, culture, or health system.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


