Hadrien Winiszewski, Thibault Vieille, Pierre-Grégoire Guinot, Nicolas Nesseler, Mael Le Berre, Laure Crognier, Anne-Claude Roche, Jean-Luc Fellahi, Nicolas D’Ostrevy, Zied Ltaief, Juliette Didier, Osama Abou Arab, Simon Meslin, Vincent Scherrer, Guillaume Besch, Alexandra Monnier, Gael Piton, Antoine Kimmoun, Gilles Capellier
{"title":"心源性休克静脉-动脉 ECMO 支持期间的氧合管理:一项多中心回顾性队列研究","authors":"Hadrien Winiszewski, Thibault Vieille, Pierre-Grégoire Guinot, Nicolas Nesseler, Mael Le Berre, Laure Crognier, Anne-Claude Roche, Jean-Luc Fellahi, Nicolas D’Ostrevy, Zied Ltaief, Juliette Didier, Osama Abou Arab, Simon Meslin, Vincent Scherrer, Guillaume Besch, Alexandra Monnier, Gael Piton, Antoine Kimmoun, Gilles Capellier","doi":"10.1186/s13613-024-01286-2","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Backgound</h3><p>Hyperoxemia is common and associated with poor outcome during veno-arterial extracorporeal membrane oxygenation (VA ECMO) support for cardiogenic shock. However, little is known about practical daily management of oxygenation. Then, we aim to describe sweep gas oxygen fraction (F<sub>S</sub>O<sub>2</sub>), postoxygenator oxygen partial pressure (P<sub>POST</sub>O<sub>2</sub>), inspired oxygen fraction (F<sub>I</sub>O<sub>2</sub>), and right radial arterial oxygen partial pressure (P<sub>a</sub>O<sub>2</sub>) between day 1 and day 7 of peripheral VA ECMO support. We also aim to evaluate the association between oxygenation parameters and outcome. In this retrospective multicentric study, each participating center had to report data on the last 10 eligible patients for whom the ICU stay was terminated. Patients with extracorporeal cardiopulmonary resuscitation were excluded. Primary endpoint was individual mean F<sub>S</sub>O<sub>2</sub> during the seven first days of ECMO support (F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub>).</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Between August 2019 and March 2022, 139 patients were enrolled in 14 ECMO centers in France, and one in Switzerland. Among them, the median value for F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> was 70 [57; 79] % but varied according to center case volume. Compared to high volume centers, centers with less than 30 VA-ECMO runs per year were more likely to maintain F<sub>S</sub>O<sub>2</sub> ≥ 70% (OR 5.04, CI 95% [1.39; 20.4], <i>p</i> = 0.017). Median value for right radial P<sub>a</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> was 114 [92; 145] mmHg, and decreased from 125 [86; 207] mmHg at day 1, to 97 [81; 133] mmHg at day 3 (<i>p</i> < 0.01). Severe hyperoxemia (i.e. right radial P<sub>a</sub>O<sub>2</sub> ≥ 300 mmHg) occurred in 16 patients (12%). P<sub>POST</sub>O<sub>2</sub>, a surrogate of the lower body oxygenation, was measured in only 39 patients (28%) among four centers. The median value of P<sub>POST</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> value was 198 [169; 231] mmHg. By multivariate analysis, age (OR 1.07, CI95% [1.03–1.11], <i>p</i> < 0.001), F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub>(OR 1.03 [1.00-1.06], <i>p</i> = 0.039), and right radial P<sub>a</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub> (OR 1.03, CI95% [1.00-1.02], <i>p</i> = 0.023) were associated with in-ICU mortality.</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>In a multicentric cohort of cardiogenic shock supported by VA ECMO, the median value for F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> was 70 [57; 79] %. P<sub>POST</sub>O<sub>2</sub> monitoring was infrequent and revealed significant hyperoxemia. Higher F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub> and right radial P<sub>a</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub> were independently associated with in-ICU mortality.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"51 1","pages":""},"PeriodicalIF":5.7000,"publicationDate":"2024-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Oxygenation management during veno-arterial ECMO support for cardiogenic shock: a multicentric retrospective cohort study\",\"authors\":\"Hadrien Winiszewski, Thibault Vieille, Pierre-Grégoire Guinot, Nicolas Nesseler, Mael Le Berre, Laure Crognier, Anne-Claude Roche, Jean-Luc Fellahi, Nicolas D’Ostrevy, Zied Ltaief, Juliette Didier, Osama Abou Arab, Simon Meslin, Vincent Scherrer, Guillaume Besch, Alexandra Monnier, Gael Piton, Antoine Kimmoun, Gilles Capellier\",\"doi\":\"10.1186/s13613-024-01286-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Backgound</h3><p>Hyperoxemia is common and associated with poor outcome during veno-arterial extracorporeal membrane oxygenation (VA ECMO) support for cardiogenic shock. However, little is known about practical daily management of oxygenation. Then, we aim to describe sweep gas oxygen fraction (F<sub>S</sub>O<sub>2</sub>), postoxygenator oxygen partial pressure (P<sub>POST</sub>O<sub>2</sub>), inspired oxygen fraction (F<sub>I</sub>O<sub>2</sub>), and right radial arterial oxygen partial pressure (P<sub>a</sub>O<sub>2</sub>) between day 1 and day 7 of peripheral VA ECMO support. We also aim to evaluate the association between oxygenation parameters and outcome. In this retrospective multicentric study, each participating center had to report data on the last 10 eligible patients for whom the ICU stay was terminated. Patients with extracorporeal cardiopulmonary resuscitation were excluded. Primary endpoint was individual mean F<sub>S</sub>O<sub>2</sub> during the seven first days of ECMO support (F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub>).</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>Between August 2019 and March 2022, 139 patients were enrolled in 14 ECMO centers in France, and one in Switzerland. Among them, the median value for F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> was 70 [57; 79] % but varied according to center case volume. Compared to high volume centers, centers with less than 30 VA-ECMO runs per year were more likely to maintain F<sub>S</sub>O<sub>2</sub> ≥ 70% (OR 5.04, CI 95% [1.39; 20.4], <i>p</i> = 0.017). Median value for right radial P<sub>a</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> was 114 [92; 145] mmHg, and decreased from 125 [86; 207] mmHg at day 1, to 97 [81; 133] mmHg at day 3 (<i>p</i> < 0.01). Severe hyperoxemia (i.e. right radial P<sub>a</sub>O<sub>2</sub> ≥ 300 mmHg) occurred in 16 patients (12%). P<sub>POST</sub>O<sub>2</sub>, a surrogate of the lower body oxygenation, was measured in only 39 patients (28%) among four centers. The median value of P<sub>POST</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> value was 198 [169; 231] mmHg. By multivariate analysis, age (OR 1.07, CI95% [1.03–1.11], <i>p</i> < 0.001), F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub>(OR 1.03 [1.00-1.06], <i>p</i> = 0.039), and right radial P<sub>a</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub> (OR 1.03, CI95% [1.00-1.02], <i>p</i> = 0.023) were associated with in-ICU mortality.</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusion</h3><p>In a multicentric cohort of cardiogenic shock supported by VA ECMO, the median value for F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−7)</i></sub> was 70 [57; 79] %. P<sub>POST</sub>O<sub>2</sub> monitoring was infrequent and revealed significant hyperoxemia. Higher F<sub>S</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub> and right radial P<sub>a</sub>O<sub>2</sub> <sub><i>mean (day 1−3)</i></sub> were independently associated with in-ICU mortality.</p>\",\"PeriodicalId\":7966,\"journal\":{\"name\":\"Annals of Intensive Care\",\"volume\":\"51 1\",\"pages\":\"\"},\"PeriodicalIF\":5.7000,\"publicationDate\":\"2024-04-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13613-024-01286-2\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-024-01286-2","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Oxygenation management during veno-arterial ECMO support for cardiogenic shock: a multicentric retrospective cohort study
Backgound
Hyperoxemia is common and associated with poor outcome during veno-arterial extracorporeal membrane oxygenation (VA ECMO) support for cardiogenic shock. However, little is known about practical daily management of oxygenation. Then, we aim to describe sweep gas oxygen fraction (FSO2), postoxygenator oxygen partial pressure (PPOSTO2), inspired oxygen fraction (FIO2), and right radial arterial oxygen partial pressure (PaO2) between day 1 and day 7 of peripheral VA ECMO support. We also aim to evaluate the association between oxygenation parameters and outcome. In this retrospective multicentric study, each participating center had to report data on the last 10 eligible patients for whom the ICU stay was terminated. Patients with extracorporeal cardiopulmonary resuscitation were excluded. Primary endpoint was individual mean FSO2 during the seven first days of ECMO support (FSO2mean (day 1−7)).
Results
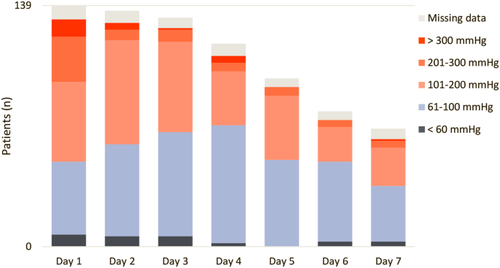
Between August 2019 and March 2022, 139 patients were enrolled in 14 ECMO centers in France, and one in Switzerland. Among them, the median value for FSO2mean (day 1−7) was 70 [57; 79] % but varied according to center case volume. Compared to high volume centers, centers with less than 30 VA-ECMO runs per year were more likely to maintain FSO2 ≥ 70% (OR 5.04, CI 95% [1.39; 20.4], p = 0.017). Median value for right radial PaO2mean (day 1−7) was 114 [92; 145] mmHg, and decreased from 125 [86; 207] mmHg at day 1, to 97 [81; 133] mmHg at day 3 (p < 0.01). Severe hyperoxemia (i.e. right radial PaO2 ≥ 300 mmHg) occurred in 16 patients (12%). PPOSTO2, a surrogate of the lower body oxygenation, was measured in only 39 patients (28%) among four centers. The median value of PPOSTO2mean (day 1−7) value was 198 [169; 231] mmHg. By multivariate analysis, age (OR 1.07, CI95% [1.03–1.11], p < 0.001), FSO2mean (day 1−3)(OR 1.03 [1.00-1.06], p = 0.039), and right radial PaO2mean (day 1−3) (OR 1.03, CI95% [1.00-1.02], p = 0.023) were associated with in-ICU mortality.
Conclusion
In a multicentric cohort of cardiogenic shock supported by VA ECMO, the median value for FSO2mean (day 1−7) was 70 [57; 79] %. PPOSTO2 monitoring was infrequent and revealed significant hyperoxemia. Higher FSO2mean (day 1−3) and right radial PaO2mean (day 1−3) were independently associated with in-ICU mortality.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


