{"title":"WEO通讯:超声评估炎症性肠病的技巧和窍门","authors":"","doi":"10.1111/den.14795","DOIUrl":null,"url":null,"abstract":"<p>Intestinal ultrasound (IUS) for inflammatory bowel disease (IBD) was described as early as 1979. However, it was not widely adopted, possibly due to the lack of proper training and concern about accuracy as compared to standard cross-sectional imaging or endoscopy. There is now renewed interest in gastroenterologist-led point-of-care ultrasound as a noninvasive, sensitive monitoring tool to assess IBD activity that is associated with excellent patient satisfaction. Current indications include suspected IBD, assessment of IBD activity and complications, monitoring therapeutic response, assessment of postoperative recurrence, and prediction of clinical outcomes.</p><p>An ultrasound machine with a low frequency curvilinear probe and a high frequency linear probe (frequency ≥7 MHz) is required to perform IUS. The low frequency probe (depth of penetration 15–22 cm) helps to detect complications such as deep-seated abscess whereas high frequency probes evaluate the bowel wall (depth 8–10 cm). The higher frequency allows higher resolution at the expense of lower penetration. Dedicated bowel ultrasound probes use single-crystal technology that, compared to the multiple Piezoelectric crystals material in conventional probes, provides higher clarity, contrast, penetration, and uniform resolution across depth.</p><p>The ultrasound machine should have dials to adjust the depth, focus, color doppler gain, contrast (dynamic range), and flow, along with the facility to measure and store still images and cine loops (Fig. 1). Increasing the depth helps to delineate deeper structures at the expense of reduced frame rate and line density. The focus dial helps to focus on a particular depth. The gain dial allows uniform amplification of the ultrasound signal by increasing the brightness of the image, and the dynamic range adjusts the shades of gray/contrast. Although increasing the contrast makes the image sharper, the smooth gradation of B (brightness)-mode imaging is compromised.</p><p>The abdomen should be exposed up to the inguinal ligament. The colon is examined starting from the left iliac fossa, identifying the iliac vessels over the left psoas muscle where the sigmoid colon is visualized (Video S1). Then the colon is traced towards the left flank to examine the descending colon and splenic flexure. Then tracing is started below the xiphisternum from the liver. The first luminal structure seen is the stomach/duodenum followed by the wavy cloud-like transverse colon with haustrations. Then the right colon can be visualized either downwards starting from the hepatic flexure just below the liver or tracing upwards from the right iliac fossa above the right iliac vessels from the terminal ileum. The small bowel is differentiated from the large bowel by the presence of peristalsis. Valvulae conniventes are seen in the jejunum which is seen in the left upper quadrant of the abdomen. The small bowel is traced using the “lawn mowing” method, in “stripes” screening vertically/horizontally along a column/row and then along the adjacent columns/rows to cover the entire abdomen.</p><p>Features to look for on IUS include bowel-wall thickness (BWT), color doppler signal (CDS) intensity, bowel-wall stratification (BWS), loss of haustration, mesenteric inflammatory fat, lymph nodes, and complications (stricture, fistula, abscess).</p><p>It is important to understand bowel-wall layers as seen on IUS. The mucosa and muscularis mucosa form a single hypoechoic innermost layer unlike that seen on endoscopic ultrasound (EUS), as ultrasound waves traverse from the skin to the bowel layer. The submucosa is hyperechoic and muscularis propria is hypoechoic. The three-layer pattern resembles an “Oreo cookie” (Fig. 2A–C). The BWT is measured from the interface of the mucosa and air inside the bowel to the interface of the muscularis propria and the serosa. The average of two measurements 1 cm apart in the longitudinal plane and two measurements 90<sup>O</sup> apart in the cross-sectional plane is considered in a given segment. BWT >3 mm is considered abnormal.</p><p>Vascularization is graded using CDS as per the modified Limberg scale (0, no vascularity; 1, few pixels visualized; 2, a stretch of doppler signals limited to bowel wall; 3, doppler signals extending to mesentery) (Fig. 3). While evaluating the vascularity of the bowel, color doppler gain should be reduced to minimize the noise with a low flow (4–6 m/s).</p><p>Bowel-wall stratification (BWS) is graded from 0 to 3 (0, no loss; 1, indeterminate; 2, <3 cm focal loss; 3 > 3 cm loss) (Fig. 4A). Inflammatory fat (i-fat) is graded as absent (0), indeterminate (1), or present (2) (Fig. 4B). Lymph nodes are measured along the short axis (Fig. 4C).</p><p>Several complications of IBD especially of Crohn's disease, such as stricture, fistula, and abscess, can be detected and evaluated (Fig. 4D–F). Stricture is defined on IUS by a narrowed lumen (<1 cm), thickened bowel wall, prestenotic dilatation (>2.5–3 cm), and hyperperistalsis.</p><p>IUS can significantly impact IBD management. The excellent agreement of IUS with colonoscopy and cross-sectional imaging findings may help to avoid those two procedures in a significant proportion of patients. Sonographic improvement precedes clinical, biochemical, and endoscopic response. Gastroenterologist-led IUS, after proper training (~200 supervised scans), has excellent agreement with and is as accurate as that performed by radiologists.<span><sup>11</sup></span></p><p>None to declare.</p><p>None.</p><p>None.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":null,"pages":null},"PeriodicalIF":5.0000,"publicationDate":"2024-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14795","citationCount":"0","resultStr":"{\"title\":\"WEO Newsletter: Tips and tricks for ultrasound assessment of inflammatory bowel disease\",\"authors\":\"\",\"doi\":\"10.1111/den.14795\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Intestinal ultrasound (IUS) for inflammatory bowel disease (IBD) was described as early as 1979. However, it was not widely adopted, possibly due to the lack of proper training and concern about accuracy as compared to standard cross-sectional imaging or endoscopy. There is now renewed interest in gastroenterologist-led point-of-care ultrasound as a noninvasive, sensitive monitoring tool to assess IBD activity that is associated with excellent patient satisfaction. Current indications include suspected IBD, assessment of IBD activity and complications, monitoring therapeutic response, assessment of postoperative recurrence, and prediction of clinical outcomes.</p><p>An ultrasound machine with a low frequency curvilinear probe and a high frequency linear probe (frequency ≥7 MHz) is required to perform IUS. The low frequency probe (depth of penetration 15–22 cm) helps to detect complications such as deep-seated abscess whereas high frequency probes evaluate the bowel wall (depth 8–10 cm). The higher frequency allows higher resolution at the expense of lower penetration. Dedicated bowel ultrasound probes use single-crystal technology that, compared to the multiple Piezoelectric crystals material in conventional probes, provides higher clarity, contrast, penetration, and uniform resolution across depth.</p><p>The ultrasound machine should have dials to adjust the depth, focus, color doppler gain, contrast (dynamic range), and flow, along with the facility to measure and store still images and cine loops (Fig. 1). Increasing the depth helps to delineate deeper structures at the expense of reduced frame rate and line density. The focus dial helps to focus on a particular depth. The gain dial allows uniform amplification of the ultrasound signal by increasing the brightness of the image, and the dynamic range adjusts the shades of gray/contrast. Although increasing the contrast makes the image sharper, the smooth gradation of B (brightness)-mode imaging is compromised.</p><p>The abdomen should be exposed up to the inguinal ligament. The colon is examined starting from the left iliac fossa, identifying the iliac vessels over the left psoas muscle where the sigmoid colon is visualized (Video S1). Then the colon is traced towards the left flank to examine the descending colon and splenic flexure. Then tracing is started below the xiphisternum from the liver. The first luminal structure seen is the stomach/duodenum followed by the wavy cloud-like transverse colon with haustrations. Then the right colon can be visualized either downwards starting from the hepatic flexure just below the liver or tracing upwards from the right iliac fossa above the right iliac vessels from the terminal ileum. The small bowel is differentiated from the large bowel by the presence of peristalsis. Valvulae conniventes are seen in the jejunum which is seen in the left upper quadrant of the abdomen. The small bowel is traced using the “lawn mowing” method, in “stripes” screening vertically/horizontally along a column/row and then along the adjacent columns/rows to cover the entire abdomen.</p><p>Features to look for on IUS include bowel-wall thickness (BWT), color doppler signal (CDS) intensity, bowel-wall stratification (BWS), loss of haustration, mesenteric inflammatory fat, lymph nodes, and complications (stricture, fistula, abscess).</p><p>It is important to understand bowel-wall layers as seen on IUS. The mucosa and muscularis mucosa form a single hypoechoic innermost layer unlike that seen on endoscopic ultrasound (EUS), as ultrasound waves traverse from the skin to the bowel layer. The submucosa is hyperechoic and muscularis propria is hypoechoic. The three-layer pattern resembles an “Oreo cookie” (Fig. 2A–C). The BWT is measured from the interface of the mucosa and air inside the bowel to the interface of the muscularis propria and the serosa. The average of two measurements 1 cm apart in the longitudinal plane and two measurements 90<sup>O</sup> apart in the cross-sectional plane is considered in a given segment. BWT >3 mm is considered abnormal.</p><p>Vascularization is graded using CDS as per the modified Limberg scale (0, no vascularity; 1, few pixels visualized; 2, a stretch of doppler signals limited to bowel wall; 3, doppler signals extending to mesentery) (Fig. 3). While evaluating the vascularity of the bowel, color doppler gain should be reduced to minimize the noise with a low flow (4–6 m/s).</p><p>Bowel-wall stratification (BWS) is graded from 0 to 3 (0, no loss; 1, indeterminate; 2, <3 cm focal loss; 3 > 3 cm loss) (Fig. 4A). Inflammatory fat (i-fat) is graded as absent (0), indeterminate (1), or present (2) (Fig. 4B). Lymph nodes are measured along the short axis (Fig. 4C).</p><p>Several complications of IBD especially of Crohn's disease, such as stricture, fistula, and abscess, can be detected and evaluated (Fig. 4D–F). Stricture is defined on IUS by a narrowed lumen (<1 cm), thickened bowel wall, prestenotic dilatation (>2.5–3 cm), and hyperperistalsis.</p><p>IUS can significantly impact IBD management. The excellent agreement of IUS with colonoscopy and cross-sectional imaging findings may help to avoid those two procedures in a significant proportion of patients. Sonographic improvement precedes clinical, biochemical, and endoscopic response. Gastroenterologist-led IUS, after proper training (~200 supervised scans), has excellent agreement with and is as accurate as that performed by radiologists.<span><sup>11</sup></span></p><p>None to declare.</p><p>None.</p><p>None.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-04-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14795\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14795\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14795","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
WEO Newsletter: Tips and tricks for ultrasound assessment of inflammatory bowel disease
Intestinal ultrasound (IUS) for inflammatory bowel disease (IBD) was described as early as 1979. However, it was not widely adopted, possibly due to the lack of proper training and concern about accuracy as compared to standard cross-sectional imaging or endoscopy. There is now renewed interest in gastroenterologist-led point-of-care ultrasound as a noninvasive, sensitive monitoring tool to assess IBD activity that is associated with excellent patient satisfaction. Current indications include suspected IBD, assessment of IBD activity and complications, monitoring therapeutic response, assessment of postoperative recurrence, and prediction of clinical outcomes.
An ultrasound machine with a low frequency curvilinear probe and a high frequency linear probe (frequency ≥7 MHz) is required to perform IUS. The low frequency probe (depth of penetration 15–22 cm) helps to detect complications such as deep-seated abscess whereas high frequency probes evaluate the bowel wall (depth 8–10 cm). The higher frequency allows higher resolution at the expense of lower penetration. Dedicated bowel ultrasound probes use single-crystal technology that, compared to the multiple Piezoelectric crystals material in conventional probes, provides higher clarity, contrast, penetration, and uniform resolution across depth.
The ultrasound machine should have dials to adjust the depth, focus, color doppler gain, contrast (dynamic range), and flow, along with the facility to measure and store still images and cine loops (Fig. 1). Increasing the depth helps to delineate deeper structures at the expense of reduced frame rate and line density. The focus dial helps to focus on a particular depth. The gain dial allows uniform amplification of the ultrasound signal by increasing the brightness of the image, and the dynamic range adjusts the shades of gray/contrast. Although increasing the contrast makes the image sharper, the smooth gradation of B (brightness)-mode imaging is compromised.
The abdomen should be exposed up to the inguinal ligament. The colon is examined starting from the left iliac fossa, identifying the iliac vessels over the left psoas muscle where the sigmoid colon is visualized (Video S1). Then the colon is traced towards the left flank to examine the descending colon and splenic flexure. Then tracing is started below the xiphisternum from the liver. The first luminal structure seen is the stomach/duodenum followed by the wavy cloud-like transverse colon with haustrations. Then the right colon can be visualized either downwards starting from the hepatic flexure just below the liver or tracing upwards from the right iliac fossa above the right iliac vessels from the terminal ileum. The small bowel is differentiated from the large bowel by the presence of peristalsis. Valvulae conniventes are seen in the jejunum which is seen in the left upper quadrant of the abdomen. The small bowel is traced using the “lawn mowing” method, in “stripes” screening vertically/horizontally along a column/row and then along the adjacent columns/rows to cover the entire abdomen.
Features to look for on IUS include bowel-wall thickness (BWT), color doppler signal (CDS) intensity, bowel-wall stratification (BWS), loss of haustration, mesenteric inflammatory fat, lymph nodes, and complications (stricture, fistula, abscess).
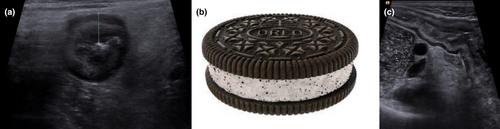
It is important to understand bowel-wall layers as seen on IUS. The mucosa and muscularis mucosa form a single hypoechoic innermost layer unlike that seen on endoscopic ultrasound (EUS), as ultrasound waves traverse from the skin to the bowel layer. The submucosa is hyperechoic and muscularis propria is hypoechoic. The three-layer pattern resembles an “Oreo cookie” (Fig. 2A–C). The BWT is measured from the interface of the mucosa and air inside the bowel to the interface of the muscularis propria and the serosa. The average of two measurements 1 cm apart in the longitudinal plane and two measurements 90O apart in the cross-sectional plane is considered in a given segment. BWT >3 mm is considered abnormal.
Vascularization is graded using CDS as per the modified Limberg scale (0, no vascularity; 1, few pixels visualized; 2, a stretch of doppler signals limited to bowel wall; 3, doppler signals extending to mesentery) (Fig. 3). While evaluating the vascularity of the bowel, color doppler gain should be reduced to minimize the noise with a low flow (4–6 m/s).
Bowel-wall stratification (BWS) is graded from 0 to 3 (0, no loss; 1, indeterminate; 2, <3 cm focal loss; 3 > 3 cm loss) (Fig. 4A). Inflammatory fat (i-fat) is graded as absent (0), indeterminate (1), or present (2) (Fig. 4B). Lymph nodes are measured along the short axis (Fig. 4C).
Several complications of IBD especially of Crohn's disease, such as stricture, fistula, and abscess, can be detected and evaluated (Fig. 4D–F). Stricture is defined on IUS by a narrowed lumen (<1 cm), thickened bowel wall, prestenotic dilatation (>2.5–3 cm), and hyperperistalsis.
IUS can significantly impact IBD management. The excellent agreement of IUS with colonoscopy and cross-sectional imaging findings may help to avoid those two procedures in a significant proportion of patients. Sonographic improvement precedes clinical, biochemical, and endoscopic response. Gastroenterologist-led IUS, after proper training (~200 supervised scans), has excellent agreement with and is as accurate as that performed by radiologists.11
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


