Ella Barrett-Chan, Li Wang, Jeffrey Bone, Amy Thachil, Kevin Vytlingam, Tom Blydt-Hansen
{"title":"利用连续尿液CXCL10/肌酐检测优化监测小儿肾移植受者异体移植物炎症的方法。","authors":"Ella Barrett-Chan, Li Wang, Jeffrey Bone, Amy Thachil, Kevin Vytlingam, Tom Blydt-Hansen","doi":"10.1111/petr.14718","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Urinary CXCL10/creatinine (uCXCL10/Cr) is proposed as an effective biomarker of subclinical rejection in pediatric kidney transplant recipients. This study objective was to model implementation in the clinical setting.</p><p><strong>Methods: </strong>Banked urine samples at a single center were tested for uCXCL10/Cr to validate published thresholds for rejection diagnosis (>80% specificity). The positive predictive value (PPV) for rejection diagnosis for uCXCL10/Cr-indicated biopsy was modeled with first-positive versus two-test-positive approaches, with accounting for changes associated with urinary tract infection (UTI), BK and CMV viremia, and subsequent recovery.</p><p><strong>Results: </strong>Seventy patients aged 10.5 ± 5.6 years at transplant (60% male) had n = 726 urine samples with n = 236 associated biopsies (no rejection = 167, borderline = 51, and Banff 1A = 18). A threshold of 12 ng/mmol was validated for Banff 1A versus no-rejection diagnosis (AUC = 0.74, 95% CI = 0.57-0.92). The first-positive test approach (n = 69) did not resolve a clinical diagnosis in 38 cases (55%), whereas the two-test approach resolved a clinical diagnosis in the majority as BK (n = 17/60, 28%), CMV (n = 4/60, 7%), UTI (n = 8/60, 13%), clinical rejection (n = 5/60, 8%), and transient elevation (n = 18, 30%). In those without a resolved clinical diagnosis, PPV from biopsy for subclinical rejection is 24% and 71% (p = .017), for first-test versus two-test models, respectively. After rejection treatment, uCXCL10/Cr level changes were all concordant with change in it-score. Sustained uCXCL10/Cr after CMV and BK viremia resolution was associated with later acute rejection.</p><p><strong>Conclusions: </strong>Urinary CXCL10/Cr reliably identifies kidney allograft inflammation. These data support a two-test approach to reliably exclude other clinically identifiable sources of inflammation, for kidney biopsy indication to rule out subclinical rejection.</p>","PeriodicalId":20038,"journal":{"name":"Pediatric Transplantation","volume":"28 3","pages":"e14718"},"PeriodicalIF":1.2000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Optimizing the approach to monitoring allograft inflammation using serial urinary CXCL10/creatinine testing in pediatric kidney transplant recipients.\",\"authors\":\"Ella Barrett-Chan, Li Wang, Jeffrey Bone, Amy Thachil, Kevin Vytlingam, Tom Blydt-Hansen\",\"doi\":\"10.1111/petr.14718\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Urinary CXCL10/creatinine (uCXCL10/Cr) is proposed as an effective biomarker of subclinical rejection in pediatric kidney transplant recipients. This study objective was to model implementation in the clinical setting.</p><p><strong>Methods: </strong>Banked urine samples at a single center were tested for uCXCL10/Cr to validate published thresholds for rejection diagnosis (>80% specificity). The positive predictive value (PPV) for rejection diagnosis for uCXCL10/Cr-indicated biopsy was modeled with first-positive versus two-test-positive approaches, with accounting for changes associated with urinary tract infection (UTI), BK and CMV viremia, and subsequent recovery.</p><p><strong>Results: </strong>Seventy patients aged 10.5 ± 5.6 years at transplant (60% male) had n = 726 urine samples with n = 236 associated biopsies (no rejection = 167, borderline = 51, and Banff 1A = 18). A threshold of 12 ng/mmol was validated for Banff 1A versus no-rejection diagnosis (AUC = 0.74, 95% CI = 0.57-0.92). The first-positive test approach (n = 69) did not resolve a clinical diagnosis in 38 cases (55%), whereas the two-test approach resolved a clinical diagnosis in the majority as BK (n = 17/60, 28%), CMV (n = 4/60, 7%), UTI (n = 8/60, 13%), clinical rejection (n = 5/60, 8%), and transient elevation (n = 18, 30%). In those without a resolved clinical diagnosis, PPV from biopsy for subclinical rejection is 24% and 71% (p = .017), for first-test versus two-test models, respectively. After rejection treatment, uCXCL10/Cr level changes were all concordant with change in it-score. Sustained uCXCL10/Cr after CMV and BK viremia resolution was associated with later acute rejection.</p><p><strong>Conclusions: </strong>Urinary CXCL10/Cr reliably identifies kidney allograft inflammation. These data support a two-test approach to reliably exclude other clinically identifiable sources of inflammation, for kidney biopsy indication to rule out subclinical rejection.</p>\",\"PeriodicalId\":20038,\"journal\":{\"name\":\"Pediatric Transplantation\",\"volume\":\"28 3\",\"pages\":\"e14718\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/petr.14718\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/petr.14718","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Optimizing the approach to monitoring allograft inflammation using serial urinary CXCL10/creatinine testing in pediatric kidney transplant recipients.
Background: Urinary CXCL10/creatinine (uCXCL10/Cr) is proposed as an effective biomarker of subclinical rejection in pediatric kidney transplant recipients. This study objective was to model implementation in the clinical setting.
Methods: Banked urine samples at a single center were tested for uCXCL10/Cr to validate published thresholds for rejection diagnosis (>80% specificity). The positive predictive value (PPV) for rejection diagnosis for uCXCL10/Cr-indicated biopsy was modeled with first-positive versus two-test-positive approaches, with accounting for changes associated with urinary tract infection (UTI), BK and CMV viremia, and subsequent recovery.
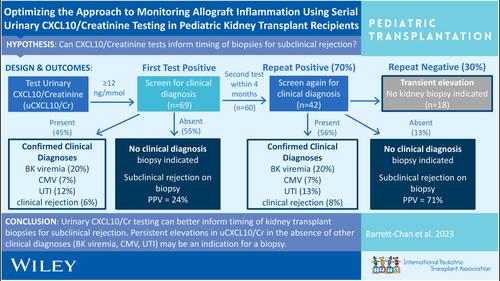
Results: Seventy patients aged 10.5 ± 5.6 years at transplant (60% male) had n = 726 urine samples with n = 236 associated biopsies (no rejection = 167, borderline = 51, and Banff 1A = 18). A threshold of 12 ng/mmol was validated for Banff 1A versus no-rejection diagnosis (AUC = 0.74, 95% CI = 0.57-0.92). The first-positive test approach (n = 69) did not resolve a clinical diagnosis in 38 cases (55%), whereas the two-test approach resolved a clinical diagnosis in the majority as BK (n = 17/60, 28%), CMV (n = 4/60, 7%), UTI (n = 8/60, 13%), clinical rejection (n = 5/60, 8%), and transient elevation (n = 18, 30%). In those without a resolved clinical diagnosis, PPV from biopsy for subclinical rejection is 24% and 71% (p = .017), for first-test versus two-test models, respectively. After rejection treatment, uCXCL10/Cr level changes were all concordant with change in it-score. Sustained uCXCL10/Cr after CMV and BK viremia resolution was associated with later acute rejection.
Conclusions: Urinary CXCL10/Cr reliably identifies kidney allograft inflammation. These data support a two-test approach to reliably exclude other clinically identifiable sources of inflammation, for kidney biopsy indication to rule out subclinical rejection.
期刊介绍:
The aim of Pediatric Transplantation is to publish original articles of the highest quality on clinical experience and basic research in transplantation of tissues and solid organs in infants, children and adolescents. The journal seeks to disseminate the latest information widely to all individuals involved in kidney, liver, heart, lung, intestine and stem cell (bone-marrow) transplantation. In addition, the journal publishes focused reviews on topics relevant to pediatric transplantation as well as timely editorial comment on controversial issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


