Terézia B Andrási, Alannah C Glück, Ildar Talipov, Lachezar Volevski, Ion Vasiloi
{"title":"针对 3v-CAD 的序列复合 BIMA 移植:预测单流入路和双流入路血管再通技术成功结果的因素。","authors":"Terézia B Andrási, Alannah C Glück, Ildar Talipov, Lachezar Volevski, Ion Vasiloi","doi":"10.1007/s11748-024-02022-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The effect of one-inflow and two-inflow coronary surgical revascularization techniques inclosing skeletonized double mammary artery (BIMA) as T-graft on outcome is studied.</p><p><strong>Methods: </strong>Early ad mid-term outcome of complete BIMA revascularization (C-T-BIMA) versus left-sided BIMA with right-sided aorto-coronary bypass (L-T-BIMA + R-CABG) is quantified and analyzed by multivariate logistic regression, Cox-regression, and Kaplan-Meier analysis in a series of 204 consecutive patients treated for triple-vessel coronary disease (3v-CAD).</p><p><strong>Results: </strong>The L-T-BIMA + R-CABG technique (n = 104) enables higher number of total (4.02 ± 0.87 vs. 3.71 ± 0.69, p = 0.015) and right-sided (1.21 ± 0.43 vs. 1.02 ± 0.32, p = 0.001) coronary anastomoses, improves total bypass flow (125.88 ± 92.41 vs. 82.50 ± 49.26 ml, p < 0.0001) and bypass flow/anastomosis (31.83 ± 23.9 vs.22.77 ± 14.23, p = 0.001), and enhances completeness of revascularization (84% vs.69%, p = 0.014) compared to C-T-BIMA strategy (n = 100), respectively. Although the incidence of MACCE was comparable in the two groups (8% vs.1.2%, p = 0.055), the progression of functional mitral regurgitation (FMR) was significantly lower after L-T-BIMA + R-CABG, then after C-T-BIMA (47% vs.64%, p = 0.017). The use of C-T-BIMA-technique (HR = 4.2, p = 0.01) and preoperative RCA occlusion (HR = 3.006, p = 0.023) predicted FMR progression, whereas L-T-Graft + R-CABG technique protected against it (X<sup>2</sup> = 14.04, p < 0.0001) independent of the anatomic and clinical complexity (Syntax score I: HR = 16.2, p = 0.156, Syntax score II: HR = 1.901, p = 0.751), of early- (0.96% vs.2%, p = 0.617) and mid-term mortality (5.8% vs.4%, p = 0.748) when compared to C-T-BIMA, respectively.</p><p><strong>Conclusions: </strong>The two-inflow coronary revascularization by L-T-BIMA + R-CABG better protects against FMR progression without increasing MACCE and mortality. Older patients with RCA occlusion and reduced LV-EF benefit most from the two-inflow L-T-BIMA + R-CABG technique. Younger 3v-CAD patients with normal LV-EF can preferentially be managed with the one-inflow C-T-BIMA; however, long-term outcome remains to be revealed.</p>","PeriodicalId":12585,"journal":{"name":"General Thoracic and Cardiovascular Surgery","volume":" ","pages":"656-667"},"PeriodicalIF":1.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11402859/pdf/","citationCount":"0","resultStr":"{\"title\":\"Sequential composite BIMA grafting for 3v-CAD: factors that predict successful outcome of the one-inflow and two-inflow revascularization techniques.\",\"authors\":\"Terézia B Andrási, Alannah C Glück, Ildar Talipov, Lachezar Volevski, Ion Vasiloi\",\"doi\":\"10.1007/s11748-024-02022-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The effect of one-inflow and two-inflow coronary surgical revascularization techniques inclosing skeletonized double mammary artery (BIMA) as T-graft on outcome is studied.</p><p><strong>Methods: </strong>Early ad mid-term outcome of complete BIMA revascularization (C-T-BIMA) versus left-sided BIMA with right-sided aorto-coronary bypass (L-T-BIMA + R-CABG) is quantified and analyzed by multivariate logistic regression, Cox-regression, and Kaplan-Meier analysis in a series of 204 consecutive patients treated for triple-vessel coronary disease (3v-CAD).</p><p><strong>Results: </strong>The L-T-BIMA + R-CABG technique (n = 104) enables higher number of total (4.02 ± 0.87 vs. 3.71 ± 0.69, p = 0.015) and right-sided (1.21 ± 0.43 vs. 1.02 ± 0.32, p = 0.001) coronary anastomoses, improves total bypass flow (125.88 ± 92.41 vs. 82.50 ± 49.26 ml, p < 0.0001) and bypass flow/anastomosis (31.83 ± 23.9 vs.22.77 ± 14.23, p = 0.001), and enhances completeness of revascularization (84% vs.69%, p = 0.014) compared to C-T-BIMA strategy (n = 100), respectively. Although the incidence of MACCE was comparable in the two groups (8% vs.1.2%, p = 0.055), the progression of functional mitral regurgitation (FMR) was significantly lower after L-T-BIMA + R-CABG, then after C-T-BIMA (47% vs.64%, p = 0.017). The use of C-T-BIMA-technique (HR = 4.2, p = 0.01) and preoperative RCA occlusion (HR = 3.006, p = 0.023) predicted FMR progression, whereas L-T-Graft + R-CABG technique protected against it (X<sup>2</sup> = 14.04, p < 0.0001) independent of the anatomic and clinical complexity (Syntax score I: HR = 16.2, p = 0.156, Syntax score II: HR = 1.901, p = 0.751), of early- (0.96% vs.2%, p = 0.617) and mid-term mortality (5.8% vs.4%, p = 0.748) when compared to C-T-BIMA, respectively.</p><p><strong>Conclusions: </strong>The two-inflow coronary revascularization by L-T-BIMA + R-CABG better protects against FMR progression without increasing MACCE and mortality. Older patients with RCA occlusion and reduced LV-EF benefit most from the two-inflow L-T-BIMA + R-CABG technique. Younger 3v-CAD patients with normal LV-EF can preferentially be managed with the one-inflow C-T-BIMA; however, long-term outcome remains to be revealed.</p>\",\"PeriodicalId\":12585,\"journal\":{\"name\":\"General Thoracic and Cardiovascular Surgery\",\"volume\":\" \",\"pages\":\"656-667\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11402859/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"General Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11748-024-02022-0\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"General Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11748-024-02022-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/20 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的研究以镂空双乳动脉(BIMA)作为 T 型移植的单流入路和双流入路冠状动脉外科血管重建技术对疗效的影响:方法:通过多变量逻辑回归、Cox回归和Kaplan-Meier分析,对204例连续接受三血管冠状动脉疾病(3v-CAD)治疗的患者进行量化,并分析完全BIMA血管再通(C-T-BIMA)与左侧BIMA加右侧主动脉旁路(L-T-BIMA + R-CABG)的早期和中期疗效:结果:L-T-BIMA + R-CABG 技术(n = 104)实现了更高的总吻合次数(4.02 ± 0.87 vs. 3.71 ± 0.69,p = 0.015)和右侧吻合次数(1.21 ± 0.43 vs. 1.02 ± 0.32,p = 0.001),改善了旁路总流量(125.88 ± 92.41 vs. 82.50 ± 49.26 ml,p 2 = 14.04,p 结论:L-T-BIMA + R-CABG 技术(n = 104)实现了更高的总吻合次数(4.02 ± 0.87 vs. 3.71 ± 0.69,p = 0.015)和右侧吻合次数(1.21 ± 0.43 vs. 1.02 ± 0.32,p = 0.001):L-T-BIMA+R-CABG的双入路冠状动脉再通术能更好地防止FMR进展,同时不会增加MACCE和死亡率。RCA闭塞和LV-EF降低的老年患者从L-T-BIMA + R-CABG双向血流技术中获益最多。左心室EF正常的年轻3V-CAD患者可优先选择单流入路C-T-BIMA;但长期疗效仍有待观察。
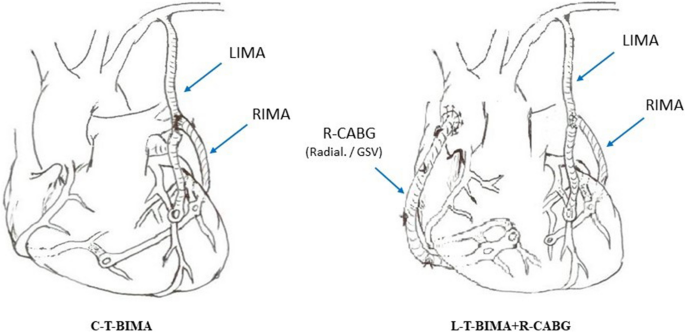
Sequential composite BIMA grafting for 3v-CAD: factors that predict successful outcome of the one-inflow and two-inflow revascularization techniques.
Objective: The effect of one-inflow and two-inflow coronary surgical revascularization techniques inclosing skeletonized double mammary artery (BIMA) as T-graft on outcome is studied.
Methods: Early ad mid-term outcome of complete BIMA revascularization (C-T-BIMA) versus left-sided BIMA with right-sided aorto-coronary bypass (L-T-BIMA + R-CABG) is quantified and analyzed by multivariate logistic regression, Cox-regression, and Kaplan-Meier analysis in a series of 204 consecutive patients treated for triple-vessel coronary disease (3v-CAD).
Results: The L-T-BIMA + R-CABG technique (n = 104) enables higher number of total (4.02 ± 0.87 vs. 3.71 ± 0.69, p = 0.015) and right-sided (1.21 ± 0.43 vs. 1.02 ± 0.32, p = 0.001) coronary anastomoses, improves total bypass flow (125.88 ± 92.41 vs. 82.50 ± 49.26 ml, p < 0.0001) and bypass flow/anastomosis (31.83 ± 23.9 vs.22.77 ± 14.23, p = 0.001), and enhances completeness of revascularization (84% vs.69%, p = 0.014) compared to C-T-BIMA strategy (n = 100), respectively. Although the incidence of MACCE was comparable in the two groups (8% vs.1.2%, p = 0.055), the progression of functional mitral regurgitation (FMR) was significantly lower after L-T-BIMA + R-CABG, then after C-T-BIMA (47% vs.64%, p = 0.017). The use of C-T-BIMA-technique (HR = 4.2, p = 0.01) and preoperative RCA occlusion (HR = 3.006, p = 0.023) predicted FMR progression, whereas L-T-Graft + R-CABG technique protected against it (X2 = 14.04, p < 0.0001) independent of the anatomic and clinical complexity (Syntax score I: HR = 16.2, p = 0.156, Syntax score II: HR = 1.901, p = 0.751), of early- (0.96% vs.2%, p = 0.617) and mid-term mortality (5.8% vs.4%, p = 0.748) when compared to C-T-BIMA, respectively.
Conclusions: The two-inflow coronary revascularization by L-T-BIMA + R-CABG better protects against FMR progression without increasing MACCE and mortality. Older patients with RCA occlusion and reduced LV-EF benefit most from the two-inflow L-T-BIMA + R-CABG technique. Younger 3v-CAD patients with normal LV-EF can preferentially be managed with the one-inflow C-T-BIMA; however, long-term outcome remains to be revealed.
期刊介绍:
The General Thoracic and Cardiovascular Surgery is the official publication of The Japanese Association for Thoracic Surgery and The Japanese Association for Chest Surgery, the affiliated journal of The Japanese Society for Cardiovascular Surgery, that publishes clinical and experimental studies in fields related to thoracic and cardiovascular surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


