{"title":"心外膜脂肪组织密度可预测心房颤动的存在及其导管消融术后的复发:三维重建图像分析。","authors":"Minoru Nodera, Tomokazu Ishida, Kanae Hasegawa, Shota Kakehashi, Moe Mukai, Daisetsu Aoyama, Shinsuke Miyazaki, Hiroyasu Uzui, Hiroshi Tada","doi":"10.1007/s00380-024-02384-8","DOIUrl":null,"url":null,"abstract":"<p><p>Epicardial adipose tissue (EAT) induces inflammation in the atria and is associated with atrial fibrillation (AF). Several studies have examined the relationship between EAT volume (EAT-V) and density (EAT-D) and the presence of AF after catheter ablation. However, conclusions have been inconsistent. This study included 43 consecutive patients who underwent catheter ablation for AF and 30 control patients. EAT-V and EAT-D around the entire heart, entire atrium, left atrium (LA), and right atrium (RA) were measured in detail using reconstructed three-dimensional (3D) EAT images from dual-source computed tomography (CT). None of the measurements of EAT-V differed significantly between patients with AF and controls or between patients with recurrent AF and those without. On the other hand, all measurements of EAT-D were higher in patients with AF than in controls (entire atrium, p < 0.001; RA, p < 0.001; LA, p = 0.002). All EAT-D measurements were associated with the presence of AF. Among patients with AF who underwent ablation, all EAT-D measurements were higher in patients with recurrent AF than in those without. The difference was significant for EATRA-D (p = 0.032). All atrial EAT-D values predicted recurrent AF (EATRA-D: hazard ratio [HR], 1.208; 95% confidence interval [95% CI], 1.053-1.387; p = 0.007; EATLA-D: HR, 1.108; 95% CI 1.001-1.225; p = 0.047; EATatrial-D: HR, 1.174; 95% CI 1.040-1.325; p = 0.010). The most sensitive cutoffs for predicting recurrent AF were highly accurate for EATRA-D (area under the curve [AUC], 0.76; p < 0.01) and EATatrial-D (AUC = 0.75, p < 0.05), while the cutoff for EATLA-D had low accuracy (AUC, 0.65; p = 0.209). For predicting the presence of AF and recurrent AF after catheter ablation, 3D analysis of atrial EAT-D, rather than EAT-V, is useful.</p>","PeriodicalId":12940,"journal":{"name":"Heart and Vessels","volume":null,"pages":null},"PeriodicalIF":1.4000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Epicardial adipose tissue density predicts the presence of atrial fibrillation and its recurrence after catheter ablation: three-dimensional reconstructed image analysis.\",\"authors\":\"Minoru Nodera, Tomokazu Ishida, Kanae Hasegawa, Shota Kakehashi, Moe Mukai, Daisetsu Aoyama, Shinsuke Miyazaki, Hiroyasu Uzui, Hiroshi Tada\",\"doi\":\"10.1007/s00380-024-02384-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Epicardial adipose tissue (EAT) induces inflammation in the atria and is associated with atrial fibrillation (AF). Several studies have examined the relationship between EAT volume (EAT-V) and density (EAT-D) and the presence of AF after catheter ablation. However, conclusions have been inconsistent. This study included 43 consecutive patients who underwent catheter ablation for AF and 30 control patients. EAT-V and EAT-D around the entire heart, entire atrium, left atrium (LA), and right atrium (RA) were measured in detail using reconstructed three-dimensional (3D) EAT images from dual-source computed tomography (CT). None of the measurements of EAT-V differed significantly between patients with AF and controls or between patients with recurrent AF and those without. On the other hand, all measurements of EAT-D were higher in patients with AF than in controls (entire atrium, p < 0.001; RA, p < 0.001; LA, p = 0.002). All EAT-D measurements were associated with the presence of AF. Among patients with AF who underwent ablation, all EAT-D measurements were higher in patients with recurrent AF than in those without. The difference was significant for EATRA-D (p = 0.032). All atrial EAT-D values predicted recurrent AF (EATRA-D: hazard ratio [HR], 1.208; 95% confidence interval [95% CI], 1.053-1.387; p = 0.007; EATLA-D: HR, 1.108; 95% CI 1.001-1.225; p = 0.047; EATatrial-D: HR, 1.174; 95% CI 1.040-1.325; p = 0.010). The most sensitive cutoffs for predicting recurrent AF were highly accurate for EATRA-D (area under the curve [AUC], 0.76; p < 0.01) and EATatrial-D (AUC = 0.75, p < 0.05), while the cutoff for EATLA-D had low accuracy (AUC, 0.65; p = 0.209). For predicting the presence of AF and recurrent AF after catheter ablation, 3D analysis of atrial EAT-D, rather than EAT-V, is useful.</p>\",\"PeriodicalId\":12940,\"journal\":{\"name\":\"Heart and Vessels\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Heart and Vessels\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00380-024-02384-8\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart and Vessels","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00380-024-02384-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Epicardial adipose tissue density predicts the presence of atrial fibrillation and its recurrence after catheter ablation: three-dimensional reconstructed image analysis.
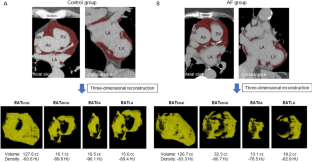
Epicardial adipose tissue (EAT) induces inflammation in the atria and is associated with atrial fibrillation (AF). Several studies have examined the relationship between EAT volume (EAT-V) and density (EAT-D) and the presence of AF after catheter ablation. However, conclusions have been inconsistent. This study included 43 consecutive patients who underwent catheter ablation for AF and 30 control patients. EAT-V and EAT-D around the entire heart, entire atrium, left atrium (LA), and right atrium (RA) were measured in detail using reconstructed three-dimensional (3D) EAT images from dual-source computed tomography (CT). None of the measurements of EAT-V differed significantly between patients with AF and controls or between patients with recurrent AF and those without. On the other hand, all measurements of EAT-D were higher in patients with AF than in controls (entire atrium, p < 0.001; RA, p < 0.001; LA, p = 0.002). All EAT-D measurements were associated with the presence of AF. Among patients with AF who underwent ablation, all EAT-D measurements were higher in patients with recurrent AF than in those without. The difference was significant for EATRA-D (p = 0.032). All atrial EAT-D values predicted recurrent AF (EATRA-D: hazard ratio [HR], 1.208; 95% confidence interval [95% CI], 1.053-1.387; p = 0.007; EATLA-D: HR, 1.108; 95% CI 1.001-1.225; p = 0.047; EATatrial-D: HR, 1.174; 95% CI 1.040-1.325; p = 0.010). The most sensitive cutoffs for predicting recurrent AF were highly accurate for EATRA-D (area under the curve [AUC], 0.76; p < 0.01) and EATatrial-D (AUC = 0.75, p < 0.05), while the cutoff for EATLA-D had low accuracy (AUC, 0.65; p = 0.209). For predicting the presence of AF and recurrent AF after catheter ablation, 3D analysis of atrial EAT-D, rather than EAT-V, is useful.
期刊介绍:
Heart and Vessels is an English-language journal that provides a forum of original ideas, excellent methods, and fascinating techniques on cardiovascular disease fields. All papers submitted for publication are evaluated only with regard to scientific quality and relevance to the heart and vessels. Contributions from those engaged in practical medicine, as well as from those involved in basic research, are welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


