{"title":"现成的骨髓间充质干细胞对小儿类固醇难治性急性移植物抗宿主病的疗效。","authors":"Hirohito Kubota, Yuki Arakawa, Yoshitaka Mizushima, Tomoya Irikura, Mai Watakabe, Takahiro Ishikawa, Ryota Kaneko, Mamoru Honda, Yuichi Mitani, Kohei Fukuoka, Makiko Mori, Koichi Oshima, Katsuyoshi Koh","doi":"10.31547/bct-2023-020","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Temcell is a mesenchymal stem cell (MSC) product approved for steroid-refractory acute graft-versus-host disease (SR-aGVHD) in Japan. However, reports regarding Temcell's efficacy in pediatric patients have been scarce, and the appropriate use of MSC therapy against pediatric SR-aGVHD also remains to be determined.</p><p><strong>Patients and methods: </strong>We retrospectively assessed a cohort of pediatric patients treated with Temcell for SR-aGVHD following allogeneic hematopoietic transplantation. MSCs were infused intravenously at a dose of 2 × 10<sup>6</sup> cells/kg according to the manufacturer's instructions.</p><p><strong>Results: </strong>Twelve patients received eighteen cycles of MSC therapy (median age, 10.3 [1.7-17.8] years), with four receiving additional cycles (one cycle: n = 3, three cycles: n = 1). The severity of aGVHD before MSC therapy was grade I-II in three patients and grade III-IV in nine patients (gut stage 3-4, n= 7; liver stage 3-4; n =2). The median number of immunosuppressive therapy regimens received prior to MSC administration was two (range: 1-5). The first MSC cycle displayed the best overall response rate of 83%, including six patients with a complete response (CR) and with a 49% reduction in the mean daily dose of prednisone after eight weeks. The median time to first response was 3.5 days (range: 2-15 days). Two of the four patients who were re-administered MSCs for recurrent or persistent GVHD achieved a CR. The three-year overall survival rate was 69.4%, while the three-year failure free survival (FFS) rate was 22.2%, with a median FFS of 4.9 months. There were no observable side effects of MSC therapy.</p><p><strong>Conclusions: </strong>MSC therapy appears to be an effective and safe treatment for pediatric SR-aGVHD, with a steroid-sparing effect and satisfactory efficacy upon re-administration. Further studies are needed to determine its appropriate combination with additional treatments and the optimal use of re-administration of MSCs.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"7 1","pages":"1-9"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10937086/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy of off-the-shelf bone marrow mesenchymal stem cells for pediatric steroid-refractory acute graft-versus-host disease.\",\"authors\":\"Hirohito Kubota, Yuki Arakawa, Yoshitaka Mizushima, Tomoya Irikura, Mai Watakabe, Takahiro Ishikawa, Ryota Kaneko, Mamoru Honda, Yuichi Mitani, Kohei Fukuoka, Makiko Mori, Koichi Oshima, Katsuyoshi Koh\",\"doi\":\"10.31547/bct-2023-020\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Temcell is a mesenchymal stem cell (MSC) product approved for steroid-refractory acute graft-versus-host disease (SR-aGVHD) in Japan. However, reports regarding Temcell's efficacy in pediatric patients have been scarce, and the appropriate use of MSC therapy against pediatric SR-aGVHD also remains to be determined.</p><p><strong>Patients and methods: </strong>We retrospectively assessed a cohort of pediatric patients treated with Temcell for SR-aGVHD following allogeneic hematopoietic transplantation. MSCs were infused intravenously at a dose of 2 × 10<sup>6</sup> cells/kg according to the manufacturer's instructions.</p><p><strong>Results: </strong>Twelve patients received eighteen cycles of MSC therapy (median age, 10.3 [1.7-17.8] years), with four receiving additional cycles (one cycle: n = 3, three cycles: n = 1). The severity of aGVHD before MSC therapy was grade I-II in three patients and grade III-IV in nine patients (gut stage 3-4, n= 7; liver stage 3-4; n =2). The median number of immunosuppressive therapy regimens received prior to MSC administration was two (range: 1-5). The first MSC cycle displayed the best overall response rate of 83%, including six patients with a complete response (CR) and with a 49% reduction in the mean daily dose of prednisone after eight weeks. The median time to first response was 3.5 days (range: 2-15 days). Two of the four patients who were re-administered MSCs for recurrent or persistent GVHD achieved a CR. The three-year overall survival rate was 69.4%, while the three-year failure free survival (FFS) rate was 22.2%, with a median FFS of 4.9 months. There were no observable side effects of MSC therapy.</p><p><strong>Conclusions: </strong>MSC therapy appears to be an effective and safe treatment for pediatric SR-aGVHD, with a steroid-sparing effect and satisfactory efficacy upon re-administration. Further studies are needed to determine its appropriate combination with additional treatments and the optimal use of re-administration of MSCs.</p>\",\"PeriodicalId\":72423,\"journal\":{\"name\":\"Blood cell therapy\",\"volume\":\"7 1\",\"pages\":\"1-9\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-12-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10937086/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31547/bct-2023-020\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/25 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2023-020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/25 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Efficacy of off-the-shelf bone marrow mesenchymal stem cells for pediatric steroid-refractory acute graft-versus-host disease.
Introduction: Temcell is a mesenchymal stem cell (MSC) product approved for steroid-refractory acute graft-versus-host disease (SR-aGVHD) in Japan. However, reports regarding Temcell's efficacy in pediatric patients have been scarce, and the appropriate use of MSC therapy against pediatric SR-aGVHD also remains to be determined.
Patients and methods: We retrospectively assessed a cohort of pediatric patients treated with Temcell for SR-aGVHD following allogeneic hematopoietic transplantation. MSCs were infused intravenously at a dose of 2 × 106 cells/kg according to the manufacturer's instructions.
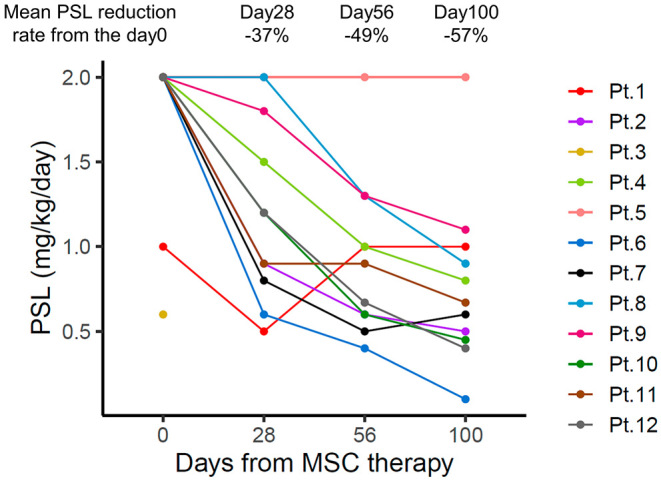
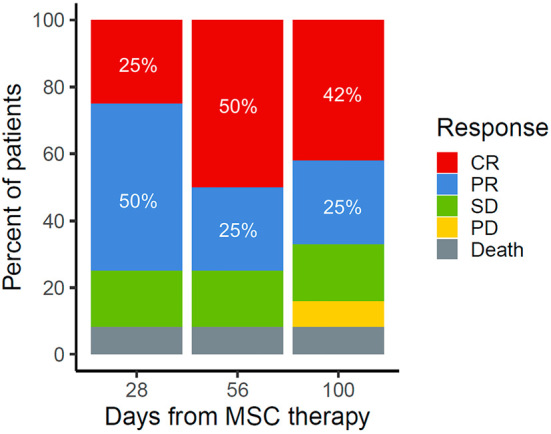
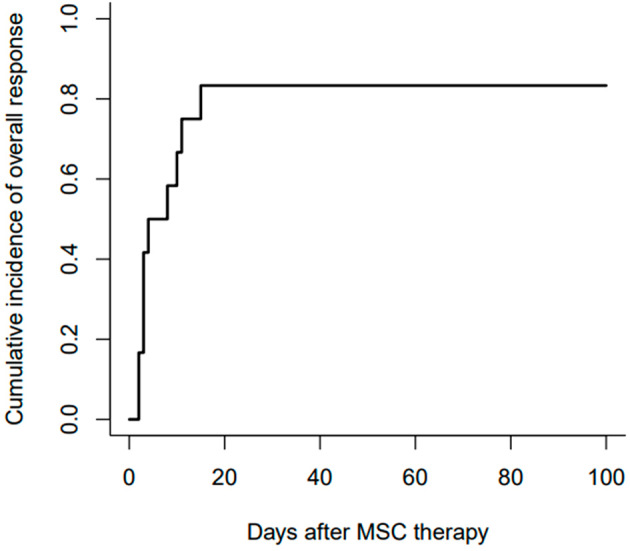
Results: Twelve patients received eighteen cycles of MSC therapy (median age, 10.3 [1.7-17.8] years), with four receiving additional cycles (one cycle: n = 3, three cycles: n = 1). The severity of aGVHD before MSC therapy was grade I-II in three patients and grade III-IV in nine patients (gut stage 3-4, n= 7; liver stage 3-4; n =2). The median number of immunosuppressive therapy regimens received prior to MSC administration was two (range: 1-5). The first MSC cycle displayed the best overall response rate of 83%, including six patients with a complete response (CR) and with a 49% reduction in the mean daily dose of prednisone after eight weeks. The median time to first response was 3.5 days (range: 2-15 days). Two of the four patients who were re-administered MSCs for recurrent or persistent GVHD achieved a CR. The three-year overall survival rate was 69.4%, while the three-year failure free survival (FFS) rate was 22.2%, with a median FFS of 4.9 months. There were no observable side effects of MSC therapy.
Conclusions: MSC therapy appears to be an effective and safe treatment for pediatric SR-aGVHD, with a steroid-sparing effect and satisfactory efficacy upon re-administration. Further studies are needed to determine its appropriate combination with additional treatments and the optimal use of re-administration of MSCs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


