Dominik M Mehler, Matthias Kreuzer, David P Obert, Luis F Cardenas, Ignacio Barra, Fernando Zurita, Francisco A Lobo, Stephan Kratzer, Gerhard Schneider, Pablo O Sepúlveda
{"title":"在老年人群中使用或不使用右美托咪定进行脑电图引导的丙泊酚-瑞芬太尼 TCI 麻醉:脑电图特征和临床评估。","authors":"Dominik M Mehler, Matthias Kreuzer, David P Obert, Luis F Cardenas, Ignacio Barra, Fernando Zurita, Francisco A Lobo, Stephan Kratzer, Gerhard Schneider, Pablo O Sepúlveda","doi":"10.1007/s10877-024-01127-4","DOIUrl":null,"url":null,"abstract":"<p><p>Elderly and multimorbid patients are at high risk for developing unfavorable postoperative neurocognitive outcomes; however, well-adjusted and EEG-guided anesthesia may help titrate anesthesia and improve postoperative outcomes. Over the last decade, dexmedetomidine has been increasingly used as an adjunct in the perioperative setting. Its synergistic effect with propofol decreases the dose of propofol needed to induce and maintain general anesthesia. In this pilot study, we evaluate two highly standardized anesthetic regimens for their potential to prevent burst suppression and postoperative neurocognitive dysfunction in a high-risk population. Prospective, randomized clinical trial with non-blinded intervention. Operating room and post anesthesia care unit at Hospital Base San José, Osorno/Universidad Austral, Valdivia, Chile. 23 patients with scheduled non-neurologic, non-cardiac surgeries with age > 69 years and a planned intervention time > 60 min. Patients were randomly assigned to receive either a propofol-remifentanil based anesthesia or an anesthetic regimen with dexmedetomidine-propofol-remifentanil. All patients underwent a slow titrated induction, followed by a target controlled infusion (TCI) of propofol and remifentanil (n = 10) or propofol, remifentanil and continuous dexmedetomidine infusion (n = 13). We compared the perioperative EEG signatures, drug-induced changes, and neurocognitive outcomes between two anesthetic regimens in geriatric patients. We conducted a pre- and postoperative Montreal Cognitive Assessment (MoCa) test and measured the level of alertness postoperatively using a sedation agitation scale to assess neurocognitive status. During slow induction, maintenance, and emergence, burst suppression was not observed in either group; however, EEG signatures differed significantly between the two groups. In general, EEG activity in the propofol group was dominated by faster rhythms than in the dexmedetomidine group. Time to responsiveness was not significantly different between the two groups (p = 0.352). Finally, no significant differences were found in postoperative cognitive outcomes evaluated by the MoCa test nor sedation agitation scale up to one hour after extubation. This pilot study demonstrates that the two proposed anesthetic regimens can be safely used to slowly induce anesthesia and avoid EEG burst suppression patterns. Despite the patients being elderly and at high risk, we did not observe postoperative neurocognitive deficits. The reduced alpha power in the dexmedetomidine-treated group was not associated with adverse neurocognitive outcomes.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"803-815"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Electroencephalographic guided propofol-remifentanil TCI anesthesia with and without dexmedetomidine in a geriatric population: electroencephalographic signatures and clinical evaluation.\",\"authors\":\"Dominik M Mehler, Matthias Kreuzer, David P Obert, Luis F Cardenas, Ignacio Barra, Fernando Zurita, Francisco A Lobo, Stephan Kratzer, Gerhard Schneider, Pablo O Sepúlveda\",\"doi\":\"10.1007/s10877-024-01127-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Elderly and multimorbid patients are at high risk for developing unfavorable postoperative neurocognitive outcomes; however, well-adjusted and EEG-guided anesthesia may help titrate anesthesia and improve postoperative outcomes. Over the last decade, dexmedetomidine has been increasingly used as an adjunct in the perioperative setting. Its synergistic effect with propofol decreases the dose of propofol needed to induce and maintain general anesthesia. In this pilot study, we evaluate two highly standardized anesthetic regimens for their potential to prevent burst suppression and postoperative neurocognitive dysfunction in a high-risk population. Prospective, randomized clinical trial with non-blinded intervention. Operating room and post anesthesia care unit at Hospital Base San José, Osorno/Universidad Austral, Valdivia, Chile. 23 patients with scheduled non-neurologic, non-cardiac surgeries with age > 69 years and a planned intervention time > 60 min. Patients were randomly assigned to receive either a propofol-remifentanil based anesthesia or an anesthetic regimen with dexmedetomidine-propofol-remifentanil. All patients underwent a slow titrated induction, followed by a target controlled infusion (TCI) of propofol and remifentanil (n = 10) or propofol, remifentanil and continuous dexmedetomidine infusion (n = 13). We compared the perioperative EEG signatures, drug-induced changes, and neurocognitive outcomes between two anesthetic regimens in geriatric patients. We conducted a pre- and postoperative Montreal Cognitive Assessment (MoCa) test and measured the level of alertness postoperatively using a sedation agitation scale to assess neurocognitive status. During slow induction, maintenance, and emergence, burst suppression was not observed in either group; however, EEG signatures differed significantly between the two groups. In general, EEG activity in the propofol group was dominated by faster rhythms than in the dexmedetomidine group. Time to responsiveness was not significantly different between the two groups (p = 0.352). Finally, no significant differences were found in postoperative cognitive outcomes evaluated by the MoCa test nor sedation agitation scale up to one hour after extubation. This pilot study demonstrates that the two proposed anesthetic regimens can be safely used to slowly induce anesthesia and avoid EEG burst suppression patterns. Despite the patients being elderly and at high risk, we did not observe postoperative neurocognitive deficits. The reduced alpha power in the dexmedetomidine-treated group was not associated with adverse neurocognitive outcomes.</p>\",\"PeriodicalId\":15513,\"journal\":{\"name\":\"Journal of Clinical Monitoring and Computing\",\"volume\":\" \",\"pages\":\"803-815\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Monitoring and Computing\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10877-024-01127-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01127-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
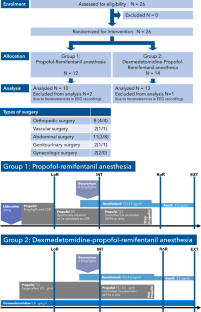
老年患者和多病患者术后出现神经认知功能障碍的风险很高;然而,在脑电图的指导下进行合理的麻醉可有助于调整麻醉剂量并改善术后效果。在过去十年中,右美托咪定越来越多地被用作围手术期的辅助用药。右美托咪定与异丙酚的协同作用可减少诱导和维持全身麻醉所需的异丙酚剂量。在这项试验性研究中,我们对两种高度标准化的麻醉方案进行了评估,以了解它们在高风险人群中预防爆发抑制和术后神经认知功能障碍的潜力。前瞻性随机临床试验,非盲干预。地点:智利瓦尔迪维亚奥索尔诺圣何塞基地医院(Hospital Base San José)/奥斯特拉尔大学(Universidad Austral)手术室和麻醉后护理病房。23 名年龄大于 69 岁、计划干预时间大于 60 分钟的非神经、非心脏手术患者。患者被随机分配接受异丙酚-瑞芬太尼麻醉或右美托咪定-异丙酚-瑞芬太尼麻醉方案。所有患者都接受了缓慢滴定诱导,然后接受异丙酚和瑞芬太尼(10 人)或异丙酚、瑞芬太尼和右美托咪定持续输注(13 人)的目标控制输注(TCI)。我们比较了两种麻醉方案在老年患者围手术期的脑电图特征、药物诱导的变化和神经认知结果。我们进行了术前和术后蒙特利尔认知评估(MoCa)测试,并使用镇静躁动量表测量了术后的警觉程度,以评估神经认知状态。在缓慢诱导、维持和唤醒过程中,两组患者均未观察到爆发抑制;但是,两组患者的脑电图特征存在显著差异。一般来说,与右美托咪定组相比,异丙酚组的脑电图活动以较快的节律为主。两组的反应时间无明显差异(p = 0.352)。最后,通过 MoCa 测试或镇静躁动量表评估的术后认知结果在拔管后一小时内无明显差异。这项试验性研究表明,所提出的两种麻醉方案可以安全地用于缓慢诱导麻醉,并避免出现脑电图爆发抑制模式。尽管患者是高龄和高危人群,但我们并未观察到术后神经认知障碍。右美托咪定治疗组的α功率降低与不良神经认知结果无关。
Electroencephalographic guided propofol-remifentanil TCI anesthesia with and without dexmedetomidine in a geriatric population: electroencephalographic signatures and clinical evaluation.
Elderly and multimorbid patients are at high risk for developing unfavorable postoperative neurocognitive outcomes; however, well-adjusted and EEG-guided anesthesia may help titrate anesthesia and improve postoperative outcomes. Over the last decade, dexmedetomidine has been increasingly used as an adjunct in the perioperative setting. Its synergistic effect with propofol decreases the dose of propofol needed to induce and maintain general anesthesia. In this pilot study, we evaluate two highly standardized anesthetic regimens for their potential to prevent burst suppression and postoperative neurocognitive dysfunction in a high-risk population. Prospective, randomized clinical trial with non-blinded intervention. Operating room and post anesthesia care unit at Hospital Base San José, Osorno/Universidad Austral, Valdivia, Chile. 23 patients with scheduled non-neurologic, non-cardiac surgeries with age > 69 years and a planned intervention time > 60 min. Patients were randomly assigned to receive either a propofol-remifentanil based anesthesia or an anesthetic regimen with dexmedetomidine-propofol-remifentanil. All patients underwent a slow titrated induction, followed by a target controlled infusion (TCI) of propofol and remifentanil (n = 10) or propofol, remifentanil and continuous dexmedetomidine infusion (n = 13). We compared the perioperative EEG signatures, drug-induced changes, and neurocognitive outcomes between two anesthetic regimens in geriatric patients. We conducted a pre- and postoperative Montreal Cognitive Assessment (MoCa) test and measured the level of alertness postoperatively using a sedation agitation scale to assess neurocognitive status. During slow induction, maintenance, and emergence, burst suppression was not observed in either group; however, EEG signatures differed significantly between the two groups. In general, EEG activity in the propofol group was dominated by faster rhythms than in the dexmedetomidine group. Time to responsiveness was not significantly different between the two groups (p = 0.352). Finally, no significant differences were found in postoperative cognitive outcomes evaluated by the MoCa test nor sedation agitation scale up to one hour after extubation. This pilot study demonstrates that the two proposed anesthetic regimens can be safely used to slowly induce anesthesia and avoid EEG burst suppression patterns. Despite the patients being elderly and at high risk, we did not observe postoperative neurocognitive deficits. The reduced alpha power in the dexmedetomidine-treated group was not associated with adverse neurocognitive outcomes.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


