Jon Jin Kim, Laura Lawless, David Marshall, Andrew Maxted, Andrew Lunn, Meeta Mallik, Alun Williams
{"title":"Envarsus 在小儿肾移植受者中的药代动力学--第一阶段试点转换研究。","authors":"Jon Jin Kim, Laura Lawless, David Marshall, Andrew Maxted, Andrew Lunn, Meeta Mallik, Alun Williams","doi":"10.1111/petr.14703","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Tacrolimus is the standard immunosuppressant for pediatric kidney transplants and is routinely administered twice daily (BD-tac). Envarsus (LCP-tac), an extended-release formulation, is approved for adults but not for pediatric patients.</p><p><strong>Methods: </strong>We conducted a pilot open-label phase 1 study in stable pediatric kidney transplant recipients (age < 18 at the time of study). Our primary objective was to compare the pharmacokinetics (Pk) of LCP-tac versus BD-tac. We conducted two 24-h Pk studies: pre-conversion (BD-tac) and 4 weeks post-conversion to LCP-tac. Patients were followed for 6 months, with the option to continue LCP-tac.</p><p><strong>Results: </strong>Five patients completed the study, with no returns to BD-tac. Median age was 15 years (range 11-17). LCP-tac exhibited an extended-release profile versus the bimodal profile of BD-tac. Time to maximum concentration was delayed (5 h vs. 1 h), and maximum concentration was lower (9.9 ng/mL vs. 14.4 ng/mL). Tacrolimus area under the curve (24 h) was comparable (141 ± 46.5 ng/mL vs. 164 ± 27.8 ng/mL). No new safety concerns arose. There were no rejection and no difference in eGFR at the study's end (1.5 mL/min/1.73 m<sup>2</sup> , range - 1.7 to 2.3 mL/min/1.73 m<sup>2</sup> ). Concentration/dose ratio was higher in LCP-tac (1.8 ± 0.64 vs. 0.8 ± 0.39). The final conversion ratio was 0.6 (BD-tac: LCP-tac).</p><p><strong>Conclusion: </strong>Our pilot study confirms the extended-release Pk profile and improved absorption of LCP-tac compared to BD-tac. A larger study is needed to further evaluate the population Pk characteristics in children.</p>","PeriodicalId":20038,"journal":{"name":"Pediatric Transplantation","volume":"28 2","pages":"e14703"},"PeriodicalIF":1.2000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Pharmacokinetics of Envarsus in pediatric kidney transplant recipients - phase 1 pilot conversion study.\",\"authors\":\"Jon Jin Kim, Laura Lawless, David Marshall, Andrew Maxted, Andrew Lunn, Meeta Mallik, Alun Williams\",\"doi\":\"10.1111/petr.14703\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Tacrolimus is the standard immunosuppressant for pediatric kidney transplants and is routinely administered twice daily (BD-tac). Envarsus (LCP-tac), an extended-release formulation, is approved for adults but not for pediatric patients.</p><p><strong>Methods: </strong>We conducted a pilot open-label phase 1 study in stable pediatric kidney transplant recipients (age < 18 at the time of study). Our primary objective was to compare the pharmacokinetics (Pk) of LCP-tac versus BD-tac. We conducted two 24-h Pk studies: pre-conversion (BD-tac) and 4 weeks post-conversion to LCP-tac. Patients were followed for 6 months, with the option to continue LCP-tac.</p><p><strong>Results: </strong>Five patients completed the study, with no returns to BD-tac. Median age was 15 years (range 11-17). LCP-tac exhibited an extended-release profile versus the bimodal profile of BD-tac. Time to maximum concentration was delayed (5 h vs. 1 h), and maximum concentration was lower (9.9 ng/mL vs. 14.4 ng/mL). Tacrolimus area under the curve (24 h) was comparable (141 ± 46.5 ng/mL vs. 164 ± 27.8 ng/mL). No new safety concerns arose. There were no rejection and no difference in eGFR at the study's end (1.5 mL/min/1.73 m<sup>2</sup> , range - 1.7 to 2.3 mL/min/1.73 m<sup>2</sup> ). Concentration/dose ratio was higher in LCP-tac (1.8 ± 0.64 vs. 0.8 ± 0.39). The final conversion ratio was 0.6 (BD-tac: LCP-tac).</p><p><strong>Conclusion: </strong>Our pilot study confirms the extended-release Pk profile and improved absorption of LCP-tac compared to BD-tac. A larger study is needed to further evaluate the population Pk characteristics in children.</p>\",\"PeriodicalId\":20038,\"journal\":{\"name\":\"Pediatric Transplantation\",\"volume\":\"28 2\",\"pages\":\"e14703\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/petr.14703\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/petr.14703","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Pharmacokinetics of Envarsus in pediatric kidney transplant recipients - phase 1 pilot conversion study.
Introduction: Tacrolimus is the standard immunosuppressant for pediatric kidney transplants and is routinely administered twice daily (BD-tac). Envarsus (LCP-tac), an extended-release formulation, is approved for adults but not for pediatric patients.
Methods: We conducted a pilot open-label phase 1 study in stable pediatric kidney transplant recipients (age < 18 at the time of study). Our primary objective was to compare the pharmacokinetics (Pk) of LCP-tac versus BD-tac. We conducted two 24-h Pk studies: pre-conversion (BD-tac) and 4 weeks post-conversion to LCP-tac. Patients were followed for 6 months, with the option to continue LCP-tac.
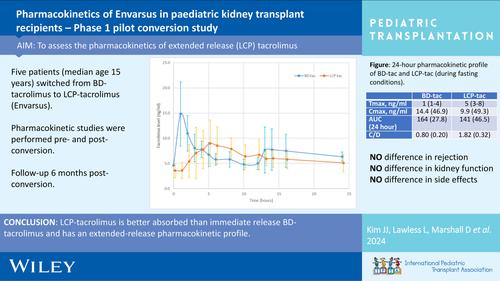
Results: Five patients completed the study, with no returns to BD-tac. Median age was 15 years (range 11-17). LCP-tac exhibited an extended-release profile versus the bimodal profile of BD-tac. Time to maximum concentration was delayed (5 h vs. 1 h), and maximum concentration was lower (9.9 ng/mL vs. 14.4 ng/mL). Tacrolimus area under the curve (24 h) was comparable (141 ± 46.5 ng/mL vs. 164 ± 27.8 ng/mL). No new safety concerns arose. There were no rejection and no difference in eGFR at the study's end (1.5 mL/min/1.73 m2 , range - 1.7 to 2.3 mL/min/1.73 m2 ). Concentration/dose ratio was higher in LCP-tac (1.8 ± 0.64 vs. 0.8 ± 0.39). The final conversion ratio was 0.6 (BD-tac: LCP-tac).
Conclusion: Our pilot study confirms the extended-release Pk profile and improved absorption of LCP-tac compared to BD-tac. A larger study is needed to further evaluate the population Pk characteristics in children.
期刊介绍:
The aim of Pediatric Transplantation is to publish original articles of the highest quality on clinical experience and basic research in transplantation of tissues and solid organs in infants, children and adolescents. The journal seeks to disseminate the latest information widely to all individuals involved in kidney, liver, heart, lung, intestine and stem cell (bone-marrow) transplantation. In addition, the journal publishes focused reviews on topics relevant to pediatric transplantation as well as timely editorial comment on controversial issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


