{"title":"β-catenin免疫染色阳性的多发性肝母细胞瘤是种系APC基因检测的潜在适应症:病例报告。","authors":"Takeshi Sato, Chihiro Takata, Jumpei Ito, Hiroyuki Shimada, Tomonobu Hasegawa","doi":"10.1111/cga.12556","DOIUrl":null,"url":null,"abstract":"<p>Germline <i>APC</i> pathogenic variants (PVs) are found in around 5%–10% of patients with hepatoblastoma.<span><sup>1</sup></span> Previous studies have shown conflicting opinion about the necessity of the routine genetic testing to identify germline <i>APC</i> PVs.<span><sup>1</sup></span> To date, candidates for genetic testing and appropriate analysis method remain unknown. Here, we experienced an infantile case of multiple hepatoblastomas with β-catenin positivity and identified a germline <i>APC</i> PV.</p><p>Our patient was the second child of healthy parents. His parents and elder brother, aged 3 years old, had no history of hepatoblastoma or adenomatous polyposis (Figure 1A). At the age of 1 year, he presented with abdominal distention and poor feeding. A huge mass was palpable in his upper right abdomen. The blood test showed high alpha-fetoprotein level (96,129 ng/mL, reference 10–50). Abdominal contrast-enhanced magnetic resonance imaging revealed three liver lesions, which size were almost 1.2 cm in S4 area, 13.0 cm in S5-6 area, and 3.0 cm in S7 area (Figure 1B,C). Multiple hepatoblastomas were diagnosed. No metastasis or vascular infiltrations were seen. After the chemotherapy, a right lobectomy was performed. Pathological examination of the resected main tumor showed a cord-like structure of small atypical cells, which is similar to the fetal liver cells, confirming hepatoblastoma. Immunohistochemistry staining showed positive β-catenin in the nuclei of tumor cells (Figure 1D). After obtaining written consent from the patient's parents for genetic testing, we performed next-generation sequencing in tumor samples and found a previously reported heterozygous nonsense variant, <i>APC</i> (NM_000038.6) c.3340C > T, p.Arg1114*.<span><sup>2</sup></span> This variant was also identified in the peripheral blood by Sanger sequencing. This variant was not identified in either parent (Figure 1A). We shared with his parents the following information: (i) this germline <i>APC</i> variant caused hepatoblastoma in our patient, (ii) due to the potential risk for additional hepatoblastoma, regular checkups were strongly recommended, (iii) our patient may develop a less severe type of adenomatous polyposis from adolescence,<span><sup>2</sup></span> and (iv) this germline <i>APC</i> variant may cause other diseases, including brain tumors and osteoma.</p><p>Multiple lesions in identical organs are common in patients with cancer predisposing genetic background. We speculate that multiple hepatoblastomas could be also suggestive of the presence of the germline PVs. We detected positive β-catenin immunostaining in the nuclei of tumor cells in our patient. Previous studies showed (i) in hepatoblastomas with β-catenin positivity, tumor-driving <i>CTNNB1</i> or <i>APC</i> variants were found in a mutually exclusive nature, (ii) somatic activating <i>CTNNB1</i> variants are found in 60%–80% of hepatoblastomas, while somatic <i>APC</i> PVs are rarely found, (iii) only a few germline <i>CTNNB1</i> variants have been reported in patients with colorectal adenomas, and (iv) the cases with germline <i>APC</i> PVs had much more lesions compared to the cases without.<span><sup>3</sup></span> Thus, it is reasonable to examine germline <i>APC</i> PVs in patients who have multiple hepatoblastomas with positive β-catenin immunostaining.</p><p>There are two potential benefits of identifying an <i>APC</i> germline PV. First, we may assess the risk of developing additional hepatoblastomas in the residual liver after the surgical treatment for primary hepatoblastoma. Theoretically, the residual liver tissues would have much higher risk of hepatoblastoma than general population. Second, we may predict the severity of colorectal polyposis during adolescence and adulthood based on <i>APC</i> PVs, although the correlation between hepatoblastoma-associated <i>APC</i> PVs and the severity of colorectal polyposis is not fully understood. <i>APC</i> p.Gln999* causes hepatoblastoma as well as classic familial adenomatous polyposis, while the severity of colorectal polyposis of <i>APC</i> p.Arg1114* in our patient is not well known. Thus, identification of <i>APC</i> PVs helps us to plan management in the short and long term.</p><p>Hepatoblastoma-related variants are clustered 5′ from codon 1309 in <i>APC</i><span><sup>4</sup></span> and can be analyzed by Sanger sequencing, which is rapid and relatively low-cost, compared to next-generation sequencing. Patients with hepatoblastoma rarely have exon deletion or entire gene deletion in <i>APC</i>. These imply that Sanger sequencing on limited area of <i>APC</i> is feasible to screen germline <i>APC</i> PVs in hepatoblastoma.</p><p>In conclusion, patients harboring multiple hepatoblastomas with positive β-catenin immunostaining may be candidates for germline <i>APC</i> testing. Also, Sanger sequencing may be appropriate screening analysis method. Further studies and discussion are necessary to determine candidates for genetic testing and appropriate analysis method.</p><p>The work was supported by Novo Nordisk Pharma Ltd. and JCR Pharmaceuticals Co., Ltd.</p><p>The authors declare no conflict of interest.</p><p>This study has been approved by the ethical committee at Keio University School of Medicine (approval number: 20170130).</p>","PeriodicalId":10626,"journal":{"name":"Congenital Anomalies","volume":"64 3","pages":"161-163"},"PeriodicalIF":1.6000,"publicationDate":"2024-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cga.12556","citationCount":"0","resultStr":"{\"title\":\"Multiple hepatoblastomas with positive β-catenin immunostaining as a potential indication for germline APC genetic testing: A case report\",\"authors\":\"Takeshi Sato, Chihiro Takata, Jumpei Ito, Hiroyuki Shimada, Tomonobu Hasegawa\",\"doi\":\"10.1111/cga.12556\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Germline <i>APC</i> pathogenic variants (PVs) are found in around 5%–10% of patients with hepatoblastoma.<span><sup>1</sup></span> Previous studies have shown conflicting opinion about the necessity of the routine genetic testing to identify germline <i>APC</i> PVs.<span><sup>1</sup></span> To date, candidates for genetic testing and appropriate analysis method remain unknown. Here, we experienced an infantile case of multiple hepatoblastomas with β-catenin positivity and identified a germline <i>APC</i> PV.</p><p>Our patient was the second child of healthy parents. His parents and elder brother, aged 3 years old, had no history of hepatoblastoma or adenomatous polyposis (Figure 1A). At the age of 1 year, he presented with abdominal distention and poor feeding. A huge mass was palpable in his upper right abdomen. The blood test showed high alpha-fetoprotein level (96,129 ng/mL, reference 10–50). Abdominal contrast-enhanced magnetic resonance imaging revealed three liver lesions, which size were almost 1.2 cm in S4 area, 13.0 cm in S5-6 area, and 3.0 cm in S7 area (Figure 1B,C). Multiple hepatoblastomas were diagnosed. No metastasis or vascular infiltrations were seen. After the chemotherapy, a right lobectomy was performed. Pathological examination of the resected main tumor showed a cord-like structure of small atypical cells, which is similar to the fetal liver cells, confirming hepatoblastoma. Immunohistochemistry staining showed positive β-catenin in the nuclei of tumor cells (Figure 1D). After obtaining written consent from the patient's parents for genetic testing, we performed next-generation sequencing in tumor samples and found a previously reported heterozygous nonsense variant, <i>APC</i> (NM_000038.6) c.3340C > T, p.Arg1114*.<span><sup>2</sup></span> This variant was also identified in the peripheral blood by Sanger sequencing. This variant was not identified in either parent (Figure 1A). We shared with his parents the following information: (i) this germline <i>APC</i> variant caused hepatoblastoma in our patient, (ii) due to the potential risk for additional hepatoblastoma, regular checkups were strongly recommended, (iii) our patient may develop a less severe type of adenomatous polyposis from adolescence,<span><sup>2</sup></span> and (iv) this germline <i>APC</i> variant may cause other diseases, including brain tumors and osteoma.</p><p>Multiple lesions in identical organs are common in patients with cancer predisposing genetic background. We speculate that multiple hepatoblastomas could be also suggestive of the presence of the germline PVs. We detected positive β-catenin immunostaining in the nuclei of tumor cells in our patient. Previous studies showed (i) in hepatoblastomas with β-catenin positivity, tumor-driving <i>CTNNB1</i> or <i>APC</i> variants were found in a mutually exclusive nature, (ii) somatic activating <i>CTNNB1</i> variants are found in 60%–80% of hepatoblastomas, while somatic <i>APC</i> PVs are rarely found, (iii) only a few germline <i>CTNNB1</i> variants have been reported in patients with colorectal adenomas, and (iv) the cases with germline <i>APC</i> PVs had much more lesions compared to the cases without.<span><sup>3</sup></span> Thus, it is reasonable to examine germline <i>APC</i> PVs in patients who have multiple hepatoblastomas with positive β-catenin immunostaining.</p><p>There are two potential benefits of identifying an <i>APC</i> germline PV. First, we may assess the risk of developing additional hepatoblastomas in the residual liver after the surgical treatment for primary hepatoblastoma. Theoretically, the residual liver tissues would have much higher risk of hepatoblastoma than general population. Second, we may predict the severity of colorectal polyposis during adolescence and adulthood based on <i>APC</i> PVs, although the correlation between hepatoblastoma-associated <i>APC</i> PVs and the severity of colorectal polyposis is not fully understood. <i>APC</i> p.Gln999* causes hepatoblastoma as well as classic familial adenomatous polyposis, while the severity of colorectal polyposis of <i>APC</i> p.Arg1114* in our patient is not well known. Thus, identification of <i>APC</i> PVs helps us to plan management in the short and long term.</p><p>Hepatoblastoma-related variants are clustered 5′ from codon 1309 in <i>APC</i><span><sup>4</sup></span> and can be analyzed by Sanger sequencing, which is rapid and relatively low-cost, compared to next-generation sequencing. Patients with hepatoblastoma rarely have exon deletion or entire gene deletion in <i>APC</i>. These imply that Sanger sequencing on limited area of <i>APC</i> is feasible to screen germline <i>APC</i> PVs in hepatoblastoma.</p><p>In conclusion, patients harboring multiple hepatoblastomas with positive β-catenin immunostaining may be candidates for germline <i>APC</i> testing. Also, Sanger sequencing may be appropriate screening analysis method. Further studies and discussion are necessary to determine candidates for genetic testing and appropriate analysis method.</p><p>The work was supported by Novo Nordisk Pharma Ltd. and JCR Pharmaceuticals Co., Ltd.</p><p>The authors declare no conflict of interest.</p><p>This study has been approved by the ethical committee at Keio University School of Medicine (approval number: 20170130).</p>\",\"PeriodicalId\":10626,\"journal\":{\"name\":\"Congenital Anomalies\",\"volume\":\"64 3\",\"pages\":\"161-163\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-02-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cga.12556\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Congenital Anomalies\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cga.12556\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Congenital Anomalies","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cga.12556","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Multiple hepatoblastomas with positive β-catenin immunostaining as a potential indication for germline APC genetic testing: A case report
Germline APC pathogenic variants (PVs) are found in around 5%–10% of patients with hepatoblastoma.1 Previous studies have shown conflicting opinion about the necessity of the routine genetic testing to identify germline APC PVs.1 To date, candidates for genetic testing and appropriate analysis method remain unknown. Here, we experienced an infantile case of multiple hepatoblastomas with β-catenin positivity and identified a germline APC PV.
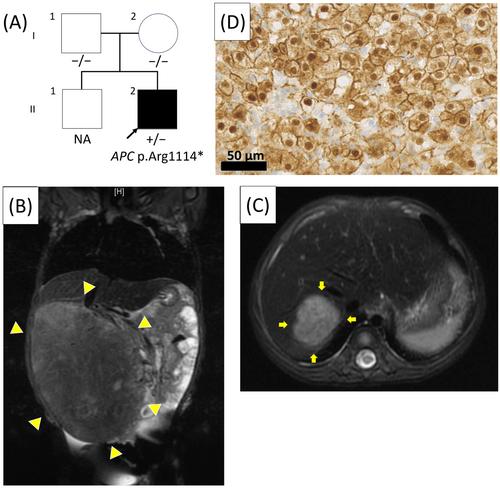
Our patient was the second child of healthy parents. His parents and elder brother, aged 3 years old, had no history of hepatoblastoma or adenomatous polyposis (Figure 1A). At the age of 1 year, he presented with abdominal distention and poor feeding. A huge mass was palpable in his upper right abdomen. The blood test showed high alpha-fetoprotein level (96,129 ng/mL, reference 10–50). Abdominal contrast-enhanced magnetic resonance imaging revealed three liver lesions, which size were almost 1.2 cm in S4 area, 13.0 cm in S5-6 area, and 3.0 cm in S7 area (Figure 1B,C). Multiple hepatoblastomas were diagnosed. No metastasis or vascular infiltrations were seen. After the chemotherapy, a right lobectomy was performed. Pathological examination of the resected main tumor showed a cord-like structure of small atypical cells, which is similar to the fetal liver cells, confirming hepatoblastoma. Immunohistochemistry staining showed positive β-catenin in the nuclei of tumor cells (Figure 1D). After obtaining written consent from the patient's parents for genetic testing, we performed next-generation sequencing in tumor samples and found a previously reported heterozygous nonsense variant, APC (NM_000038.6) c.3340C > T, p.Arg1114*.2 This variant was also identified in the peripheral blood by Sanger sequencing. This variant was not identified in either parent (Figure 1A). We shared with his parents the following information: (i) this germline APC variant caused hepatoblastoma in our patient, (ii) due to the potential risk for additional hepatoblastoma, regular checkups were strongly recommended, (iii) our patient may develop a less severe type of adenomatous polyposis from adolescence,2 and (iv) this germline APC variant may cause other diseases, including brain tumors and osteoma.
Multiple lesions in identical organs are common in patients with cancer predisposing genetic background. We speculate that multiple hepatoblastomas could be also suggestive of the presence of the germline PVs. We detected positive β-catenin immunostaining in the nuclei of tumor cells in our patient. Previous studies showed (i) in hepatoblastomas with β-catenin positivity, tumor-driving CTNNB1 or APC variants were found in a mutually exclusive nature, (ii) somatic activating CTNNB1 variants are found in 60%–80% of hepatoblastomas, while somatic APC PVs are rarely found, (iii) only a few germline CTNNB1 variants have been reported in patients with colorectal adenomas, and (iv) the cases with germline APC PVs had much more lesions compared to the cases without.3 Thus, it is reasonable to examine germline APC PVs in patients who have multiple hepatoblastomas with positive β-catenin immunostaining.
There are two potential benefits of identifying an APC germline PV. First, we may assess the risk of developing additional hepatoblastomas in the residual liver after the surgical treatment for primary hepatoblastoma. Theoretically, the residual liver tissues would have much higher risk of hepatoblastoma than general population. Second, we may predict the severity of colorectal polyposis during adolescence and adulthood based on APC PVs, although the correlation between hepatoblastoma-associated APC PVs and the severity of colorectal polyposis is not fully understood. APC p.Gln999* causes hepatoblastoma as well as classic familial adenomatous polyposis, while the severity of colorectal polyposis of APC p.Arg1114* in our patient is not well known. Thus, identification of APC PVs helps us to plan management in the short and long term.
Hepatoblastoma-related variants are clustered 5′ from codon 1309 in APC4 and can be analyzed by Sanger sequencing, which is rapid and relatively low-cost, compared to next-generation sequencing. Patients with hepatoblastoma rarely have exon deletion or entire gene deletion in APC. These imply that Sanger sequencing on limited area of APC is feasible to screen germline APC PVs in hepatoblastoma.
In conclusion, patients harboring multiple hepatoblastomas with positive β-catenin immunostaining may be candidates for germline APC testing. Also, Sanger sequencing may be appropriate screening analysis method. Further studies and discussion are necessary to determine candidates for genetic testing and appropriate analysis method.
The work was supported by Novo Nordisk Pharma Ltd. and JCR Pharmaceuticals Co., Ltd.
The authors declare no conflict of interest.
This study has been approved by the ethical committee at Keio University School of Medicine (approval number: 20170130).
期刊介绍:
Congenital Anomalies is the official English language journal of the Japanese Teratology Society, and publishes original articles in laboratory as well as clinical research in all areas of abnormal development and related fields, from all over the world. Although contributions by members of the teratology societies affiliated with The International Federation of Teratology Societies are given priority, contributions from non-members are welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


