{"title":"快速发展的黑色素瘤术前和术后系统治疗。","authors":"Ryan C. Augustin, Jason J. Luke","doi":"10.1007/s40257-024-00852-5","DOIUrl":null,"url":null,"abstract":"<div><p>With the development of effective <i>BRAF</i>-targeted and immune-checkpoint immunotherapies for metastatic melanoma, clinical trials are moving these treatments into earlier adjuvant and perioperative settings. <i>BRAF</i>-targeted therapy is a standard of care in resected stage III–IV melanoma, while anti-programmed death-1 (PD1) immunotherapy is now a standard of care option in resected stage IIB through IV disease. With both modalities, recurrence-free survival and distant-metastasis-free survival are improved by a relative 35–50%, yet no improvement in overall survival has been demonstrated. Neoadjuvant anti-PD1 therapy improves event-free survival by approximately an absolute 23%, although improvements in overall survival have yet to be demonstrated. Understanding which patients are most likely to recur and which are most likely to benefit from treatment is now the highest priority question in the field. Biomarker analyses, such as gene expression profiling of the primary lesion and circulating DNA, are preliminarily exciting as potential biomarkers, though each has drawbacks. As in the setting of metastatic disease, markers that inform positive outcomes include interferon-<i>γ</i> gene expression, PD-L1, and high tumor mutational burden, while negative predictors of outcome include circulating factors such as lactate dehydrogenase, interleukin-8, and C-reactive protein. Integrating and validating these markers into clinically relevant models is thus a high priority. Melanoma therapeutics continues to advance with combination adjuvant approaches now investigating anti-PD1 with lymphocyte activation gene 3 (LAG3), T-cell immunoreceptor with Ig and ITIM domains (TIGIT), and individualized neoantigen therapies. How this progress will be integrated into the management of a unique patient to reduce recurrence, limit toxicity, and avoid over-treatment will dominate clinical research and patient care over the next decade.</p></div>","PeriodicalId":7706,"journal":{"name":"American Journal of Clinical Dermatology","volume":"25 3","pages":"421 - 434"},"PeriodicalIF":8.6000,"publicationDate":"2024-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Rapidly Evolving Pre- and Post-surgical Systemic Treatment of Melanoma\",\"authors\":\"Ryan C. Augustin, Jason J. Luke\",\"doi\":\"10.1007/s40257-024-00852-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>With the development of effective <i>BRAF</i>-targeted and immune-checkpoint immunotherapies for metastatic melanoma, clinical trials are moving these treatments into earlier adjuvant and perioperative settings. <i>BRAF</i>-targeted therapy is a standard of care in resected stage III–IV melanoma, while anti-programmed death-1 (PD1) immunotherapy is now a standard of care option in resected stage IIB through IV disease. With both modalities, recurrence-free survival and distant-metastasis-free survival are improved by a relative 35–50%, yet no improvement in overall survival has been demonstrated. Neoadjuvant anti-PD1 therapy improves event-free survival by approximately an absolute 23%, although improvements in overall survival have yet to be demonstrated. Understanding which patients are most likely to recur and which are most likely to benefit from treatment is now the highest priority question in the field. Biomarker analyses, such as gene expression profiling of the primary lesion and circulating DNA, are preliminarily exciting as potential biomarkers, though each has drawbacks. As in the setting of metastatic disease, markers that inform positive outcomes include interferon-<i>γ</i> gene expression, PD-L1, and high tumor mutational burden, while negative predictors of outcome include circulating factors such as lactate dehydrogenase, interleukin-8, and C-reactive protein. Integrating and validating these markers into clinically relevant models is thus a high priority. Melanoma therapeutics continues to advance with combination adjuvant approaches now investigating anti-PD1 with lymphocyte activation gene 3 (LAG3), T-cell immunoreceptor with Ig and ITIM domains (TIGIT), and individualized neoantigen therapies. How this progress will be integrated into the management of a unique patient to reduce recurrence, limit toxicity, and avoid over-treatment will dominate clinical research and patient care over the next decade.</p></div>\",\"PeriodicalId\":7706,\"journal\":{\"name\":\"American Journal of Clinical Dermatology\",\"volume\":\"25 3\",\"pages\":\"421 - 434\"},\"PeriodicalIF\":8.6000,\"publicationDate\":\"2024-02-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Clinical Dermatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://link.springer.com/article/10.1007/s40257-024-00852-5\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Clinical Dermatology","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s40257-024-00852-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
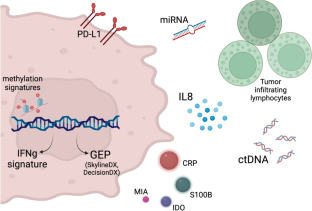
随着针对转移性黑色素瘤的有效 BRAF 靶向疗法和免疫检查点免疫疗法的开发,临床试验正在将这些疗法推向早期辅助治疗和围手术期治疗。BRAF靶向疗法是切除的III-IV期黑色素瘤的标准治疗方法,而抗程序性死亡-1(PD1)免疫疗法目前是切除的IIB期至IV期疾病的标准治疗方法。采用这两种疗法后,无复发生存期和无远处转移生存期相对提高了35%-50%,但总生存期却没有得到改善。新辅助抗PD1疗法可将无事件生存期绝对值提高约23%,但总生存期的改善尚未得到证实。了解哪些患者最有可能复发,哪些患者最有可能从治疗中获益是目前该领域最优先考虑的问题。生物标志物分析,如原发病灶和循环 DNA 的基因表达谱分析,作为潜在的生物标志物初步令人兴奋,但每种方法都有缺点。与转移性疾病的情况一样,能预测阳性结果的标志物包括干扰素-γ 基因表达、PD-L1 和高肿瘤突变负荷,而预测阴性结果的标志物包括乳酸脱氢酶、白细胞介素-8 和 C 反应蛋白等循环因子。因此,将这些标记物整合并验证到临床相关模型中是当务之急。黑色素瘤疗法也在不断进步,目前正在研究抗PD1与淋巴细胞活化基因3(LAG3)、带Ig和ITIM结构域的T细胞免疫受体(TIGIT)以及个体化新抗原疗法的联合辅助疗法。在未来十年中,如何将这些进展整合到对特殊患者的管理中,以减少复发、限制毒性并避免过度治疗,将成为临床研究和患者护理的主要方向。
Rapidly Evolving Pre- and Post-surgical Systemic Treatment of Melanoma
With the development of effective BRAF-targeted and immune-checkpoint immunotherapies for metastatic melanoma, clinical trials are moving these treatments into earlier adjuvant and perioperative settings. BRAF-targeted therapy is a standard of care in resected stage III–IV melanoma, while anti-programmed death-1 (PD1) immunotherapy is now a standard of care option in resected stage IIB through IV disease. With both modalities, recurrence-free survival and distant-metastasis-free survival are improved by a relative 35–50%, yet no improvement in overall survival has been demonstrated. Neoadjuvant anti-PD1 therapy improves event-free survival by approximately an absolute 23%, although improvements in overall survival have yet to be demonstrated. Understanding which patients are most likely to recur and which are most likely to benefit from treatment is now the highest priority question in the field. Biomarker analyses, such as gene expression profiling of the primary lesion and circulating DNA, are preliminarily exciting as potential biomarkers, though each has drawbacks. As in the setting of metastatic disease, markers that inform positive outcomes include interferon-γ gene expression, PD-L1, and high tumor mutational burden, while negative predictors of outcome include circulating factors such as lactate dehydrogenase, interleukin-8, and C-reactive protein. Integrating and validating these markers into clinically relevant models is thus a high priority. Melanoma therapeutics continues to advance with combination adjuvant approaches now investigating anti-PD1 with lymphocyte activation gene 3 (LAG3), T-cell immunoreceptor with Ig and ITIM domains (TIGIT), and individualized neoantigen therapies. How this progress will be integrated into the management of a unique patient to reduce recurrence, limit toxicity, and avoid over-treatment will dominate clinical research and patient care over the next decade.
期刊介绍:
The American Journal of Clinical Dermatology is dedicated to evidence-based therapy and effective patient management in dermatology. It publishes critical review articles and clinically focused original research covering comprehensive aspects of dermatological conditions. The journal enhances visibility and educational value through features like Key Points summaries, plain language summaries, and various digital elements, ensuring accessibility and depth for a diverse readership.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


