{"title":"口咽部大出血型心绞痛","authors":"Yuki Okubo, Mitsuhiro Matsuo, Takateru Ihara","doi":"10.1002/ams2.930","DOIUrl":null,"url":null,"abstract":"<p>A 66-year-old woman presented to the emergency department with sudden throat tightness. The patient was uncomfortable and could not speak. No pain, dysphagia, drooling, labored breathing, or snoring were noted, and she had an unremarkable medical and allergic history. Oral examination revealed a 4-cm bloody blister in the middle of the soft palate (Figure 1A). Blood examination revealed no coagulopathy or anemia.</p><p>The patient was diagnosed with angina bullosa haemorrhagica (ABH). Puncture drainage was suggested to prevent airway obstruction. Preparation for airway management, including cricothyrotomy, was performed. However, the patient's blister spontaneously ruptured, and symptoms disappeared. A shallow ulcer formed at the post-rupture site (Figure 1B).</p><p>ABH was first reported by Badham in 1967 as the rapid formation of a bloody blister on the oral mucosa.<span><sup>1</sup></span> Its diagnosis relies on the patient's clinical symptoms. Most cases of ABH are 1–2 cm in diameter, and no reports are found on a similar size to our case.<span><sup>2, 3</sup></span> Most are resolved without treatment, but several cases of airway obstruction have been reported, one of which required puncture drainage to secure the airway.<span><sup>4, 5</sup></span> Therefore, airway obstruction should be considered when large ABH in the oropharynx or severe symptoms are present.</p><p>The authors have no financial relationships relevant to this article.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: Consent was obtained from the patient in the form of British Medical Journal.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":null,"pages":null},"PeriodicalIF":1.5000,"publicationDate":"2024-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.930","citationCount":"0","resultStr":"{\"title\":\"Gigantic angina bullosa haemorrhagica in the oropharynx\",\"authors\":\"Yuki Okubo, Mitsuhiro Matsuo, Takateru Ihara\",\"doi\":\"10.1002/ams2.930\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 66-year-old woman presented to the emergency department with sudden throat tightness. The patient was uncomfortable and could not speak. No pain, dysphagia, drooling, labored breathing, or snoring were noted, and she had an unremarkable medical and allergic history. Oral examination revealed a 4-cm bloody blister in the middle of the soft palate (Figure 1A). Blood examination revealed no coagulopathy or anemia.</p><p>The patient was diagnosed with angina bullosa haemorrhagica (ABH). Puncture drainage was suggested to prevent airway obstruction. Preparation for airway management, including cricothyrotomy, was performed. However, the patient's blister spontaneously ruptured, and symptoms disappeared. A shallow ulcer formed at the post-rupture site (Figure 1B).</p><p>ABH was first reported by Badham in 1967 as the rapid formation of a bloody blister on the oral mucosa.<span><sup>1</sup></span> Its diagnosis relies on the patient's clinical symptoms. Most cases of ABH are 1–2 cm in diameter, and no reports are found on a similar size to our case.<span><sup>2, 3</sup></span> Most are resolved without treatment, but several cases of airway obstruction have been reported, one of which required puncture drainage to secure the airway.<span><sup>4, 5</sup></span> Therefore, airway obstruction should be considered when large ABH in the oropharynx or severe symptoms are present.</p><p>The authors have no financial relationships relevant to this article.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: Consent was obtained from the patient in the form of British Medical Journal.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>\",\"PeriodicalId\":7196,\"journal\":{\"name\":\"Acute Medicine & Surgery\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-02-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.930\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute Medicine & Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ams2.930\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.930","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Gigantic angina bullosa haemorrhagica in the oropharynx
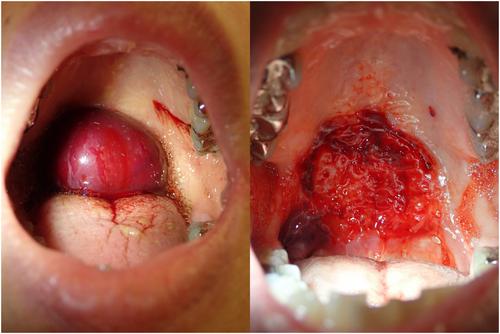
A 66-year-old woman presented to the emergency department with sudden throat tightness. The patient was uncomfortable and could not speak. No pain, dysphagia, drooling, labored breathing, or snoring were noted, and she had an unremarkable medical and allergic history. Oral examination revealed a 4-cm bloody blister in the middle of the soft palate (Figure 1A). Blood examination revealed no coagulopathy or anemia.
The patient was diagnosed with angina bullosa haemorrhagica (ABH). Puncture drainage was suggested to prevent airway obstruction. Preparation for airway management, including cricothyrotomy, was performed. However, the patient's blister spontaneously ruptured, and symptoms disappeared. A shallow ulcer formed at the post-rupture site (Figure 1B).
ABH was first reported by Badham in 1967 as the rapid formation of a bloody blister on the oral mucosa.1 Its diagnosis relies on the patient's clinical symptoms. Most cases of ABH are 1–2 cm in diameter, and no reports are found on a similar size to our case.2, 3 Most are resolved without treatment, but several cases of airway obstruction have been reported, one of which required puncture drainage to secure the airway.4, 5 Therefore, airway obstruction should be considered when large ABH in the oropharynx or severe symptoms are present.
The authors have no financial relationships relevant to this article.
Approval of the research protocol: N/A.
Informed consent: Consent was obtained from the patient in the form of British Medical Journal.
Registry and the registration no. of the study/trial: N/A.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


