{"title":"用尼拉帕利作为一线维持疗法治疗 RAD51C 突变携带者的原发性输卵管癌和原发性乳腺癌:病例报告。","authors":"Hua Yuan, Rong Zhang, Ning Li, Hongwen Yao","doi":"10.1186/s13053-024-00274-8","DOIUrl":null,"url":null,"abstract":"<p><p>Given the rarity of RAD51C mutations, the risk and treatment of metachronous breast cancer after the diagnosis of ovarian cancer in RAD51C mutation carriers is not clear, especially for those who have received PARPi treatment. We report the case of a 65-year-old woman diagnosed with stage IIIC high-grade serous primary fallopian tube cancer. The patient had no family history of breast or ovarian cancer. The patient received three cycles of neoadjuvant chemotherapy with paclitaxel and carboplatin and achieved a complete response. After interval debulking surgery, the patient received three cycles of adjuvant chemotherapy. Collection and extraction of saliva DNA for next-generation sequencing identified a RAD51C mutation c.838-2 A > G. The patient received niraparib as front-line maintenance treatment. After 36 months of niraparib treatment, the patient had grade II invasive ductal carcinoma of the left breast that was positive for estrogen receptor (90%) and Ki-67 (30%) and negative for progesterone receptor and human epidermal growth factor receptor 2. Computed tomography revealed the absence of distant metastases. Modified radical mastectomy and axillary lymph node dissection were then performed. The final pathological report of the breast showed a 1.8 cm Bloom-Richardson grade II invasive ductal carcinoma in the left breast with axillary lymph node metastasis (1/21). Finally, the breast cancer was stage IIA, pT1cN1M0. The metachronous breast cancer in this case may be the first report of second primary cancer in fallopian tube cancer patient harboring a RAD51C mutation during niraparib treatment. Further studies are required to determine optimal treatment.</p>","PeriodicalId":55058,"journal":{"name":"Hereditary Cancer in Clinical Practice","volume":"22 1","pages":"2"},"PeriodicalIF":2.4000,"publicationDate":"2024-02-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10868093/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary fallopian tube cancer followed by primary breast cancer in RAD51C mutation carrier treated with niraparib as first line maintenance therapy: a case report.\",\"authors\":\"Hua Yuan, Rong Zhang, Ning Li, Hongwen Yao\",\"doi\":\"10.1186/s13053-024-00274-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Given the rarity of RAD51C mutations, the risk and treatment of metachronous breast cancer after the diagnosis of ovarian cancer in RAD51C mutation carriers is not clear, especially for those who have received PARPi treatment. We report the case of a 65-year-old woman diagnosed with stage IIIC high-grade serous primary fallopian tube cancer. The patient had no family history of breast or ovarian cancer. The patient received three cycles of neoadjuvant chemotherapy with paclitaxel and carboplatin and achieved a complete response. After interval debulking surgery, the patient received three cycles of adjuvant chemotherapy. Collection and extraction of saliva DNA for next-generation sequencing identified a RAD51C mutation c.838-2 A > G. The patient received niraparib as front-line maintenance treatment. After 36 months of niraparib treatment, the patient had grade II invasive ductal carcinoma of the left breast that was positive for estrogen receptor (90%) and Ki-67 (30%) and negative for progesterone receptor and human epidermal growth factor receptor 2. Computed tomography revealed the absence of distant metastases. Modified radical mastectomy and axillary lymph node dissection were then performed. The final pathological report of the breast showed a 1.8 cm Bloom-Richardson grade II invasive ductal carcinoma in the left breast with axillary lymph node metastasis (1/21). Finally, the breast cancer was stage IIA, pT1cN1M0. The metachronous breast cancer in this case may be the first report of second primary cancer in fallopian tube cancer patient harboring a RAD51C mutation during niraparib treatment. Further studies are required to determine optimal treatment.</p>\",\"PeriodicalId\":55058,\"journal\":{\"name\":\"Hereditary Cancer in Clinical Practice\",\"volume\":\"22 1\",\"pages\":\"2\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-02-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10868093/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hereditary Cancer in Clinical Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13053-024-00274-8\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hereditary Cancer in Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13053-024-00274-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Primary fallopian tube cancer followed by primary breast cancer in RAD51C mutation carrier treated with niraparib as first line maintenance therapy: a case report.
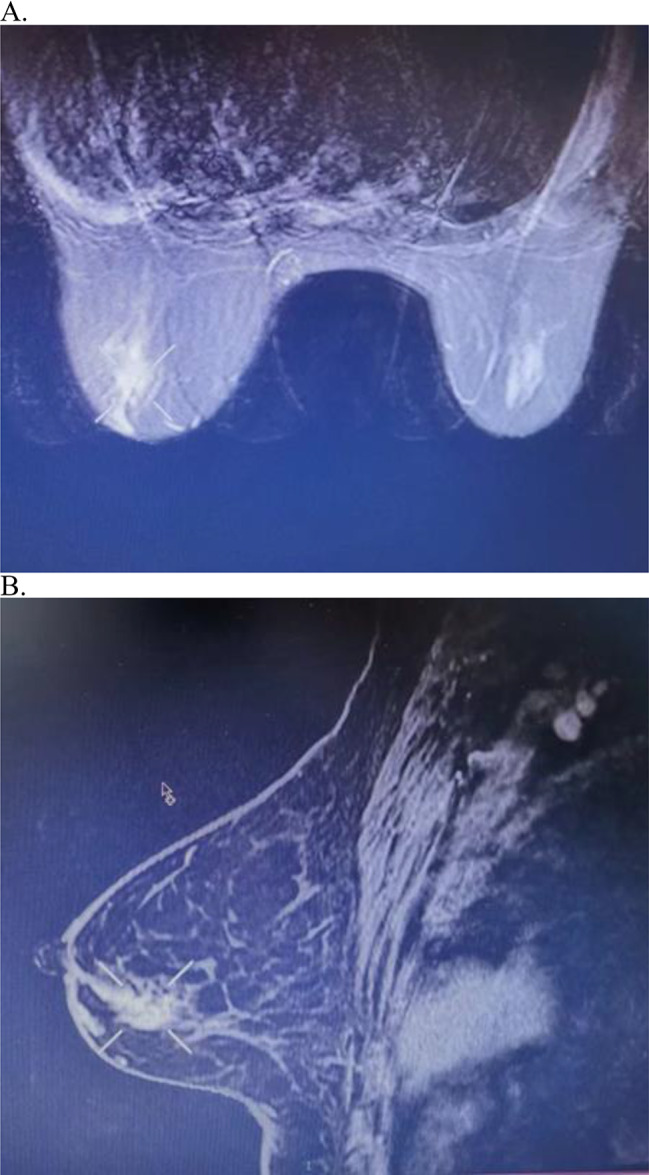
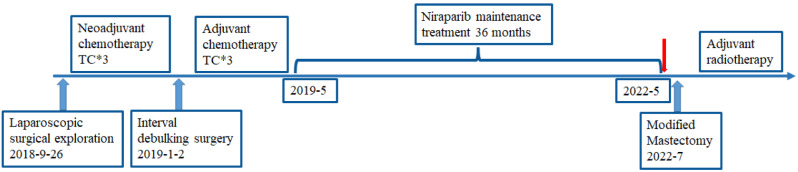
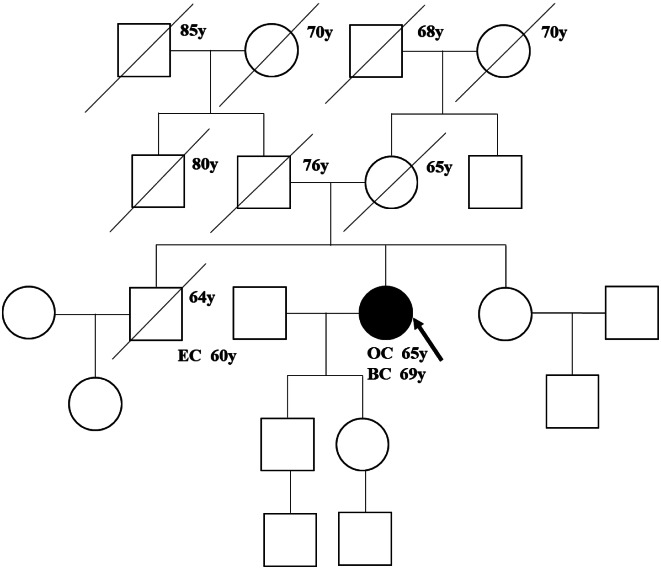
Given the rarity of RAD51C mutations, the risk and treatment of metachronous breast cancer after the diagnosis of ovarian cancer in RAD51C mutation carriers is not clear, especially for those who have received PARPi treatment. We report the case of a 65-year-old woman diagnosed with stage IIIC high-grade serous primary fallopian tube cancer. The patient had no family history of breast or ovarian cancer. The patient received three cycles of neoadjuvant chemotherapy with paclitaxel and carboplatin and achieved a complete response. After interval debulking surgery, the patient received three cycles of adjuvant chemotherapy. Collection and extraction of saliva DNA for next-generation sequencing identified a RAD51C mutation c.838-2 A > G. The patient received niraparib as front-line maintenance treatment. After 36 months of niraparib treatment, the patient had grade II invasive ductal carcinoma of the left breast that was positive for estrogen receptor (90%) and Ki-67 (30%) and negative for progesterone receptor and human epidermal growth factor receptor 2. Computed tomography revealed the absence of distant metastases. Modified radical mastectomy and axillary lymph node dissection were then performed. The final pathological report of the breast showed a 1.8 cm Bloom-Richardson grade II invasive ductal carcinoma in the left breast with axillary lymph node metastasis (1/21). Finally, the breast cancer was stage IIA, pT1cN1M0. The metachronous breast cancer in this case may be the first report of second primary cancer in fallopian tube cancer patient harboring a RAD51C mutation during niraparib treatment. Further studies are required to determine optimal treatment.
期刊介绍:
Hereditary Cancer in Clinical Practice is an open access journal that publishes articles of interest for the cancer genetics community and serves as a discussion forum for the development appropriate healthcare strategies.
Cancer genetics encompasses a wide variety of disciplines and knowledge in the field is rapidly growing, especially as the amount of information linking genetic differences to inherited cancer predispositions continues expanding. With the increased knowledge of genetic variability and how this relates to cancer risk there is a growing demand not only to disseminate this information into clinical practice but also to enable competent debate concerning how such information is managed and what it implies for patient care.
Topics covered by the journal include but are not limited to:
Original research articles on any aspect of inherited predispositions to cancer.
Reviews of inherited cancer predispositions.
Application of molecular and cytogenetic analysis to clinical decision making.
Clinical aspects of the management of hereditary cancers.
Genetic counselling issues associated with cancer genetics.
The role of registries in improving health care of patients with an inherited predisposition to cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


