Matthias Gröger, Dominik Felbel, Michael Paukovitsch, Leonhard Moritz Schneider, Sinisa Markovic, Wolfgang Rottbauer, Mirjam Keßler
{"title":"经导管边对边二尖瓣修复术后入住瓣膜病房而非重症监护病房或中级监护病房是安全的,并能减少术后并发症。","authors":"Matthias Gröger, Dominik Felbel, Michael Paukovitsch, Leonhard Moritz Schneider, Sinisa Markovic, Wolfgang Rottbauer, Mirjam Keßler","doi":"10.1007/s00392-024-02384-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transcatheter edge-to-edge mitral valve repair (M-TEER) is often performed in general anesthesia, and postprocedural monitoring is usually warranted on an intensive or intermediate care unit (ICU/IMC). We evaluated the implications of a dedicated valve unit (VU) instead of an ICU/IMC for monitoring after M-TEER.</p><p><strong>Methods and results: </strong>In total, 624 patients were retrospectively analyzed. A total of 312 patients were primarily transferred to either ICU or IMC following M-TEER, and 312 patients were scheduled for the VU in the absence of indications for ICU/IMC treatment. Hospital stay was significantly shorter in VU patients (median 6.0 days (interquartile range (IQR) 5.0 - 8.0) vs. 7.0 days (IQR 6.0 - 10.0), p < 0.001) and their risk for infections (2.9 vs. 7.7%, p = 0.008) and delirium (0.6 vs. 2.6%, p = 0.056) was substantially lower compared to ICU/IMC patients. In-hospital mortality was similar in both groups (0.6% vs. 1.3%, p = 0.41). Fifty patients (16.0%) in the VU group had to cross over to unplanned ICU/IMC admission. The most frequent indication was prolonged need for catecholamines (52.0%). Patients with ICU/IMC crossover had more advanced stages of heart failure (LV-EF < 30% in 36.0 vs. 16.0%, p = 0.001; severe concomitant tricuspid regurgitation in 48.0 vs. 27.8%, p = 0.005) and an LV-EF < 30% was independently associated with unplanned ICU/IMC admission.</p><p><strong>Conclusions: </strong>Following M-TEER postprocedural monitoring on a VU instead of an ICU/IMC is safe, reduces complications, and spares ICU capacities. Patients with advanced heart failure have a higher risk for unplanned ICU/IMC treatment after M-TEER.</p>","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":" ","pages":"818-826"},"PeriodicalIF":3.7000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202642/pdf/","citationCount":"0","resultStr":"{\"title\":\"Valve unit instead of intensive or intermediate care unit admission following transcatheter edge-to-edge mitral valve repair is safe and reduces postprocedural complications.\",\"authors\":\"Matthias Gröger, Dominik Felbel, Michael Paukovitsch, Leonhard Moritz Schneider, Sinisa Markovic, Wolfgang Rottbauer, Mirjam Keßler\",\"doi\":\"10.1007/s00392-024-02384-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Transcatheter edge-to-edge mitral valve repair (M-TEER) is often performed in general anesthesia, and postprocedural monitoring is usually warranted on an intensive or intermediate care unit (ICU/IMC). We evaluated the implications of a dedicated valve unit (VU) instead of an ICU/IMC for monitoring after M-TEER.</p><p><strong>Methods and results: </strong>In total, 624 patients were retrospectively analyzed. A total of 312 patients were primarily transferred to either ICU or IMC following M-TEER, and 312 patients were scheduled for the VU in the absence of indications for ICU/IMC treatment. Hospital stay was significantly shorter in VU patients (median 6.0 days (interquartile range (IQR) 5.0 - 8.0) vs. 7.0 days (IQR 6.0 - 10.0), p < 0.001) and their risk for infections (2.9 vs. 7.7%, p = 0.008) and delirium (0.6 vs. 2.6%, p = 0.056) was substantially lower compared to ICU/IMC patients. In-hospital mortality was similar in both groups (0.6% vs. 1.3%, p = 0.41). Fifty patients (16.0%) in the VU group had to cross over to unplanned ICU/IMC admission. The most frequent indication was prolonged need for catecholamines (52.0%). Patients with ICU/IMC crossover had more advanced stages of heart failure (LV-EF < 30% in 36.0 vs. 16.0%, p = 0.001; severe concomitant tricuspid regurgitation in 48.0 vs. 27.8%, p = 0.005) and an LV-EF < 30% was independently associated with unplanned ICU/IMC admission.</p><p><strong>Conclusions: </strong>Following M-TEER postprocedural monitoring on a VU instead of an ICU/IMC is safe, reduces complications, and spares ICU capacities. Patients with advanced heart failure have a higher risk for unplanned ICU/IMC treatment after M-TEER.</p>\",\"PeriodicalId\":10474,\"journal\":{\"name\":\"Clinical Research in Cardiology\",\"volume\":\" \",\"pages\":\"818-826\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202642/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Research in Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00392-024-02384-8\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02384-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Valve unit instead of intensive or intermediate care unit admission following transcatheter edge-to-edge mitral valve repair is safe and reduces postprocedural complications.
Background: Transcatheter edge-to-edge mitral valve repair (M-TEER) is often performed in general anesthesia, and postprocedural monitoring is usually warranted on an intensive or intermediate care unit (ICU/IMC). We evaluated the implications of a dedicated valve unit (VU) instead of an ICU/IMC for monitoring after M-TEER.
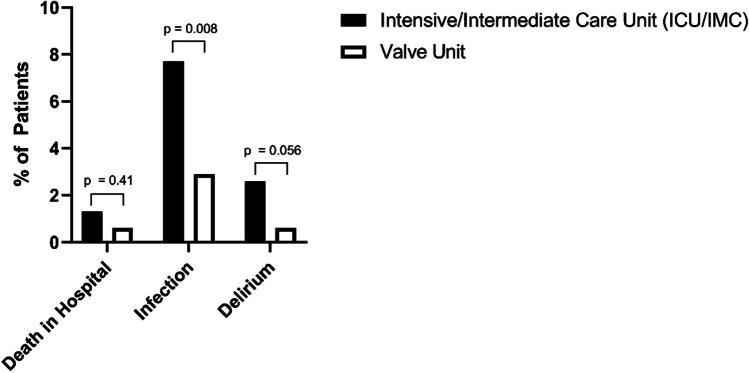
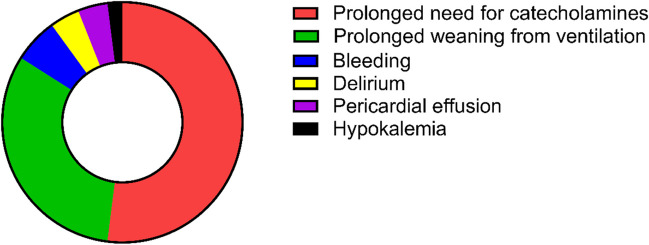
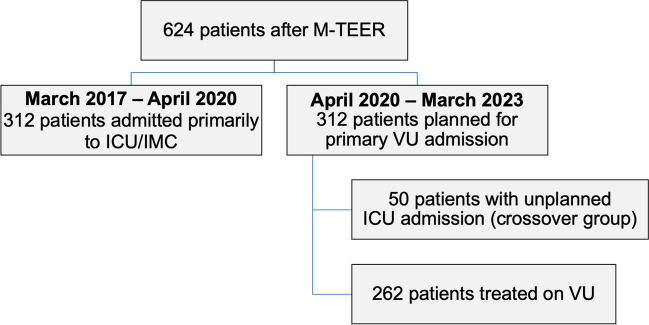
Methods and results: In total, 624 patients were retrospectively analyzed. A total of 312 patients were primarily transferred to either ICU or IMC following M-TEER, and 312 patients were scheduled for the VU in the absence of indications for ICU/IMC treatment. Hospital stay was significantly shorter in VU patients (median 6.0 days (interquartile range (IQR) 5.0 - 8.0) vs. 7.0 days (IQR 6.0 - 10.0), p < 0.001) and their risk for infections (2.9 vs. 7.7%, p = 0.008) and delirium (0.6 vs. 2.6%, p = 0.056) was substantially lower compared to ICU/IMC patients. In-hospital mortality was similar in both groups (0.6% vs. 1.3%, p = 0.41). Fifty patients (16.0%) in the VU group had to cross over to unplanned ICU/IMC admission. The most frequent indication was prolonged need for catecholamines (52.0%). Patients with ICU/IMC crossover had more advanced stages of heart failure (LV-EF < 30% in 36.0 vs. 16.0%, p = 0.001; severe concomitant tricuspid regurgitation in 48.0 vs. 27.8%, p = 0.005) and an LV-EF < 30% was independently associated with unplanned ICU/IMC admission.
Conclusions: Following M-TEER postprocedural monitoring on a VU instead of an ICU/IMC is safe, reduces complications, and spares ICU capacities. Patients with advanced heart failure have a higher risk for unplanned ICU/IMC treatment after M-TEER.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


