{"title":"非囊性纤维化支气管扩张症中耐多药细菌感染的流行病学和结果。","authors":"Chih-Hao Chang, Chiung-Hsin Chang, Shih-Hao Huang, Chung-Shu Lee, Po-Chuan Ko, Chun-Yu Lin, Meng-Heng Hsieh, Yu-Tung Huang, Horng-Chyuan Lin, Li-Fu Li, Fu-Tsai Chung, Chun-Hua Wang, Hung-Yu Huang","doi":"10.1186/s12941-024-00675-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Multidrug-resistant (MDR) bacteria impose a considerable health-care burden and are associated with bronchiectasis exacerbation. This study investigated the clinical outcomes of adult patients with bronchiectasis following MDR bacterial infection.</p><p><strong>Methods: </strong>From the Chang Gung Research Database, we identified patients with bronchiectasis and MDR bacterial infection from 2008 to 2017. The control group comprised patients with bronchiectasis who did not have MDR bacterial infection and were propensity-score matched at a 1:2 ratio. The main outcomes were in-hospital and 3-year mortality.</p><p><strong>Results: </strong>In total, 554 patients with both bronchiectasis and MDR bacterial infection were identified. The types of MDR bacteria that most commonly affected the patients were MDR- Acinetobacter baumannii (38.6%) and methicillin-resistant Staphylococcus aureus (18.4%), Extended-spectrum-beta-lactamases (ESBL)- Klebsiella pneumoniae (17.8%), MDR-Pseudomonas (14.8%), and ESBL-E. coli (7.5%). Compared with the control group, the MDR group exhibited lower body mass index scores, higher rate of chronic bacterial colonization, a higher rate of previous exacerbations, and an increased use of antibiotics. Furthermore, the MDR group exhibited a higher rate of respiratory failure during hospitalization (MDR vs. control, 41.3% vs. 12.4%; p < 0.001). The MDR and control groups exhibited in-hospital mortality rates of 26.7% and 7.6%, respectively (p < 0.001); 3-year respiratory failure rates of 33.5% and 13.5%, respectively (p < 0.001); and 3-year mortality rates of 73.3% and 41.5%, respectively (p < 0.001). After adjustments were made for confounding factors, the infection with MDR and MDR bacteria species were determined to be independent risk factors affecting in-hospital and 3-year mortality.</p><p><strong>Conclusions: </strong>MDR bacteria were discovered in patients with more severe bronchiectasis and were independently associated with an increased risk of in-hospital and 3-year mortality. Given our findings, we recommend that clinicians identify patients at risk of MDR bacterial infection and follow the principle of antimicrobial stewardship to prevent the emergence of resistant bacteria among patients with bronchiectasis.</p>","PeriodicalId":8052,"journal":{"name":"Annals of Clinical Microbiology and Antimicrobials","volume":"23 1","pages":"15"},"PeriodicalIF":3.6000,"publicationDate":"2024-02-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10865664/pdf/","citationCount":"0","resultStr":"{\"title\":\"Epidemiology and outcomes of multidrug-resistant bacterial infection in non-cystic fibrosis bronchiectasis.\",\"authors\":\"Chih-Hao Chang, Chiung-Hsin Chang, Shih-Hao Huang, Chung-Shu Lee, Po-Chuan Ko, Chun-Yu Lin, Meng-Heng Hsieh, Yu-Tung Huang, Horng-Chyuan Lin, Li-Fu Li, Fu-Tsai Chung, Chun-Hua Wang, Hung-Yu Huang\",\"doi\":\"10.1186/s12941-024-00675-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Multidrug-resistant (MDR) bacteria impose a considerable health-care burden and are associated with bronchiectasis exacerbation. This study investigated the clinical outcomes of adult patients with bronchiectasis following MDR bacterial infection.</p><p><strong>Methods: </strong>From the Chang Gung Research Database, we identified patients with bronchiectasis and MDR bacterial infection from 2008 to 2017. The control group comprised patients with bronchiectasis who did not have MDR bacterial infection and were propensity-score matched at a 1:2 ratio. The main outcomes were in-hospital and 3-year mortality.</p><p><strong>Results: </strong>In total, 554 patients with both bronchiectasis and MDR bacterial infection were identified. The types of MDR bacteria that most commonly affected the patients were MDR- Acinetobacter baumannii (38.6%) and methicillin-resistant Staphylococcus aureus (18.4%), Extended-spectrum-beta-lactamases (ESBL)- Klebsiella pneumoniae (17.8%), MDR-Pseudomonas (14.8%), and ESBL-E. coli (7.5%). Compared with the control group, the MDR group exhibited lower body mass index scores, higher rate of chronic bacterial colonization, a higher rate of previous exacerbations, and an increased use of antibiotics. Furthermore, the MDR group exhibited a higher rate of respiratory failure during hospitalization (MDR vs. control, 41.3% vs. 12.4%; p < 0.001). The MDR and control groups exhibited in-hospital mortality rates of 26.7% and 7.6%, respectively (p < 0.001); 3-year respiratory failure rates of 33.5% and 13.5%, respectively (p < 0.001); and 3-year mortality rates of 73.3% and 41.5%, respectively (p < 0.001). After adjustments were made for confounding factors, the infection with MDR and MDR bacteria species were determined to be independent risk factors affecting in-hospital and 3-year mortality.</p><p><strong>Conclusions: </strong>MDR bacteria were discovered in patients with more severe bronchiectasis and were independently associated with an increased risk of in-hospital and 3-year mortality. Given our findings, we recommend that clinicians identify patients at risk of MDR bacterial infection and follow the principle of antimicrobial stewardship to prevent the emergence of resistant bacteria among patients with bronchiectasis.</p>\",\"PeriodicalId\":8052,\"journal\":{\"name\":\"Annals of Clinical Microbiology and Antimicrobials\",\"volume\":\"23 1\",\"pages\":\"15\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-02-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10865664/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Clinical Microbiology and Antimicrobials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12941-024-00675-6\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MICROBIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Clinical Microbiology and Antimicrobials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12941-024-00675-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MICROBIOLOGY","Score":null,"Total":0}
Epidemiology and outcomes of multidrug-resistant bacterial infection in non-cystic fibrosis bronchiectasis.
Purpose: Multidrug-resistant (MDR) bacteria impose a considerable health-care burden and are associated with bronchiectasis exacerbation. This study investigated the clinical outcomes of adult patients with bronchiectasis following MDR bacterial infection.
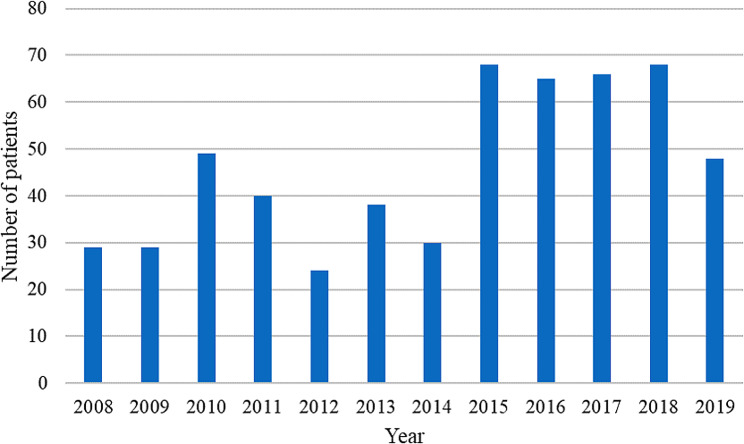
Methods: From the Chang Gung Research Database, we identified patients with bronchiectasis and MDR bacterial infection from 2008 to 2017. The control group comprised patients with bronchiectasis who did not have MDR bacterial infection and were propensity-score matched at a 1:2 ratio. The main outcomes were in-hospital and 3-year mortality.
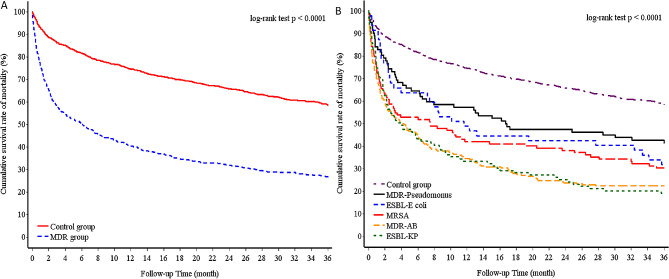
Results: In total, 554 patients with both bronchiectasis and MDR bacterial infection were identified. The types of MDR bacteria that most commonly affected the patients were MDR- Acinetobacter baumannii (38.6%) and methicillin-resistant Staphylococcus aureus (18.4%), Extended-spectrum-beta-lactamases (ESBL)- Klebsiella pneumoniae (17.8%), MDR-Pseudomonas (14.8%), and ESBL-E. coli (7.5%). Compared with the control group, the MDR group exhibited lower body mass index scores, higher rate of chronic bacterial colonization, a higher rate of previous exacerbations, and an increased use of antibiotics. Furthermore, the MDR group exhibited a higher rate of respiratory failure during hospitalization (MDR vs. control, 41.3% vs. 12.4%; p < 0.001). The MDR and control groups exhibited in-hospital mortality rates of 26.7% and 7.6%, respectively (p < 0.001); 3-year respiratory failure rates of 33.5% and 13.5%, respectively (p < 0.001); and 3-year mortality rates of 73.3% and 41.5%, respectively (p < 0.001). After adjustments were made for confounding factors, the infection with MDR and MDR bacteria species were determined to be independent risk factors affecting in-hospital and 3-year mortality.
Conclusions: MDR bacteria were discovered in patients with more severe bronchiectasis and were independently associated with an increased risk of in-hospital and 3-year mortality. Given our findings, we recommend that clinicians identify patients at risk of MDR bacterial infection and follow the principle of antimicrobial stewardship to prevent the emergence of resistant bacteria among patients with bronchiectasis.
期刊介绍:
Annals of Clinical Microbiology and Antimicrobials considers good quality, novel and international research of more than regional relevance. Research must include epidemiological and/or clinical information about isolates, and the journal covers the clinical microbiology of bacteria, viruses and fungi, as well as antimicrobial treatment of infectious diseases.
Annals of Clinical Microbiology and Antimicrobials is an open access, peer-reviewed journal focusing on information concerning clinical microbiology, infectious diseases and antimicrobials. The management of infectious disease is dependent on correct diagnosis and appropriate antimicrobial treatment, and with this in mind, the journal aims to improve the communication between laboratory and clinical science in the field of clinical microbiology and antimicrobial treatment. Furthermore, the journal has no restrictions on space or access; this ensures that the journal can reach the widest possible audience.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


