Hyungjong Park, Sung-Il Sohn, Gwang Hyun Leem, Minho Kim, Yun Hak Kim, Tae-Jin Song
{"title":"成功接受血管内血栓切除术治疗的急性缺血性脑卒中患者的标准血压控制与强化血压控制:随机对照试验的系统回顾和元分析》。","authors":"Hyungjong Park, Sung-Il Sohn, Gwang Hyun Leem, Minho Kim, Yun Hak Kim, Tae-Jin Song","doi":"10.5853/jos.2023.04119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>The optimal blood pressure (BP) control after successful endovascular thrombectomy (EVT) in acute ischemic stroke (AIS) with large vessel occlusion (LVO) remains debatable. We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) that evaluate the efficacy and safety of standard BP control (with systolic BP ≤180 mm Hg) versus intensive BP control (systolic BP <140 mm Hg) during the 24 hours after successful EVT in AIS with LVO.</p><p><strong>Methods: </strong>PubMed, Scopus, the Cochrane Central Register of Controlled Trials, and Embase were searched to identify relevant trials. The crude odds ratio (OR) and 95% confidence interval (CI) were calculated and estimates using random-effects models were pooled. This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (PROSPERO ID: CRD42023450673).</p><p><strong>Results: </strong>Four RCTs involving 1,559 participants were included. Regarding efficacy outcomes, intensive BP control was associated with a lower likelihood of functional independence (OR: 0.68; 95% CI: 0.51-0.91 for modified Rankin Scale [mRS] ≤2) and walking without assistance (OR: 0.65; 95% CI: 0.53-0.81 for mRS ≤3). For safety outcomes, consistent with the efficacy findings, intensive BP control was significantly associated with severe disability or death (mRS 5 or 6) (OR: 1.34; 95% CI: 1.07-1.69). However, there were no significant differences including all-cause mortality, any intracerebral hemorrhage (ICH), symptomatic ICH, parenchymal hematoma type 2, and stroke recurrence.</p><p><strong>Conclusion: </strong>While all four RCTs were conducted to demonstrate the superiority of intensive BP control over standard BP control, standard BP control may be beneficial for the outcome after EVT for AIS with LVO without increasing adverse safety outcomes. Caution should be needed with the application of intensive BP control during the 24 hours following successful recanalization after EVT.</p>","PeriodicalId":17135,"journal":{"name":"Journal of Stroke","volume":"26 1","pages":"54-63"},"PeriodicalIF":8.6000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10850446/pdf/","citationCount":"0","resultStr":"{\"title\":\"Standard Versus Intensive Blood Pressure Control in Acute Ischemic Stroke Patients Successfully Treated With Endovascular Thrombectomy: A Systemic Review and Meta-Analysis of Randomized Controlled Trials.\",\"authors\":\"Hyungjong Park, Sung-Il Sohn, Gwang Hyun Leem, Minho Kim, Yun Hak Kim, Tae-Jin Song\",\"doi\":\"10.5853/jos.2023.04119\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>The optimal blood pressure (BP) control after successful endovascular thrombectomy (EVT) in acute ischemic stroke (AIS) with large vessel occlusion (LVO) remains debatable. We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) that evaluate the efficacy and safety of standard BP control (with systolic BP ≤180 mm Hg) versus intensive BP control (systolic BP <140 mm Hg) during the 24 hours after successful EVT in AIS with LVO.</p><p><strong>Methods: </strong>PubMed, Scopus, the Cochrane Central Register of Controlled Trials, and Embase were searched to identify relevant trials. The crude odds ratio (OR) and 95% confidence interval (CI) were calculated and estimates using random-effects models were pooled. This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (PROSPERO ID: CRD42023450673).</p><p><strong>Results: </strong>Four RCTs involving 1,559 participants were included. Regarding efficacy outcomes, intensive BP control was associated with a lower likelihood of functional independence (OR: 0.68; 95% CI: 0.51-0.91 for modified Rankin Scale [mRS] ≤2) and walking without assistance (OR: 0.65; 95% CI: 0.53-0.81 for mRS ≤3). For safety outcomes, consistent with the efficacy findings, intensive BP control was significantly associated with severe disability or death (mRS 5 or 6) (OR: 1.34; 95% CI: 1.07-1.69). However, there were no significant differences including all-cause mortality, any intracerebral hemorrhage (ICH), symptomatic ICH, parenchymal hematoma type 2, and stroke recurrence.</p><p><strong>Conclusion: </strong>While all four RCTs were conducted to demonstrate the superiority of intensive BP control over standard BP control, standard BP control may be beneficial for the outcome after EVT for AIS with LVO without increasing adverse safety outcomes. Caution should be needed with the application of intensive BP control during the 24 hours following successful recanalization after EVT.</p>\",\"PeriodicalId\":17135,\"journal\":{\"name\":\"Journal of Stroke\",\"volume\":\"26 1\",\"pages\":\"54-63\"},\"PeriodicalIF\":8.6000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10850446/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Stroke\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5853/jos.2023.04119\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5853/jos.2023.04119","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Standard Versus Intensive Blood Pressure Control in Acute Ischemic Stroke Patients Successfully Treated With Endovascular Thrombectomy: A Systemic Review and Meta-Analysis of Randomized Controlled Trials.
Background and purpose: The optimal blood pressure (BP) control after successful endovascular thrombectomy (EVT) in acute ischemic stroke (AIS) with large vessel occlusion (LVO) remains debatable. We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) that evaluate the efficacy and safety of standard BP control (with systolic BP ≤180 mm Hg) versus intensive BP control (systolic BP <140 mm Hg) during the 24 hours after successful EVT in AIS with LVO.
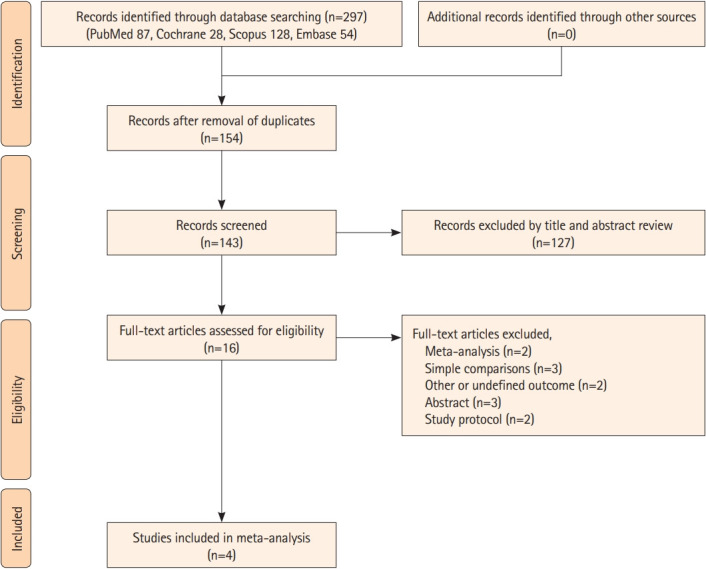
Methods: PubMed, Scopus, the Cochrane Central Register of Controlled Trials, and Embase were searched to identify relevant trials. The crude odds ratio (OR) and 95% confidence interval (CI) were calculated and estimates using random-effects models were pooled. This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (PROSPERO ID: CRD42023450673).
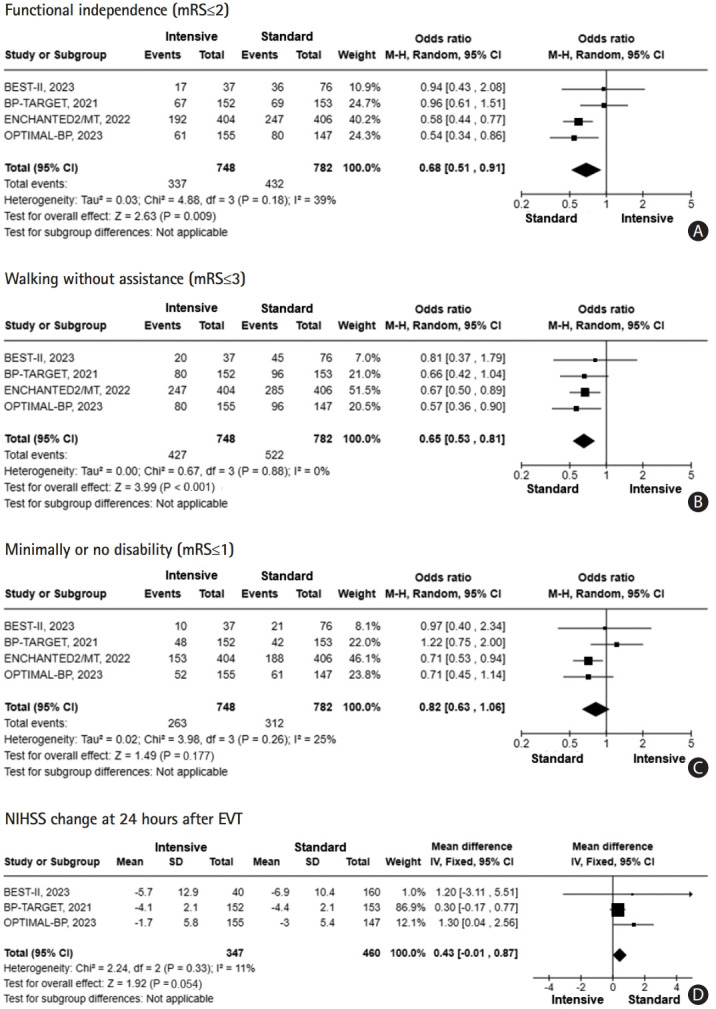
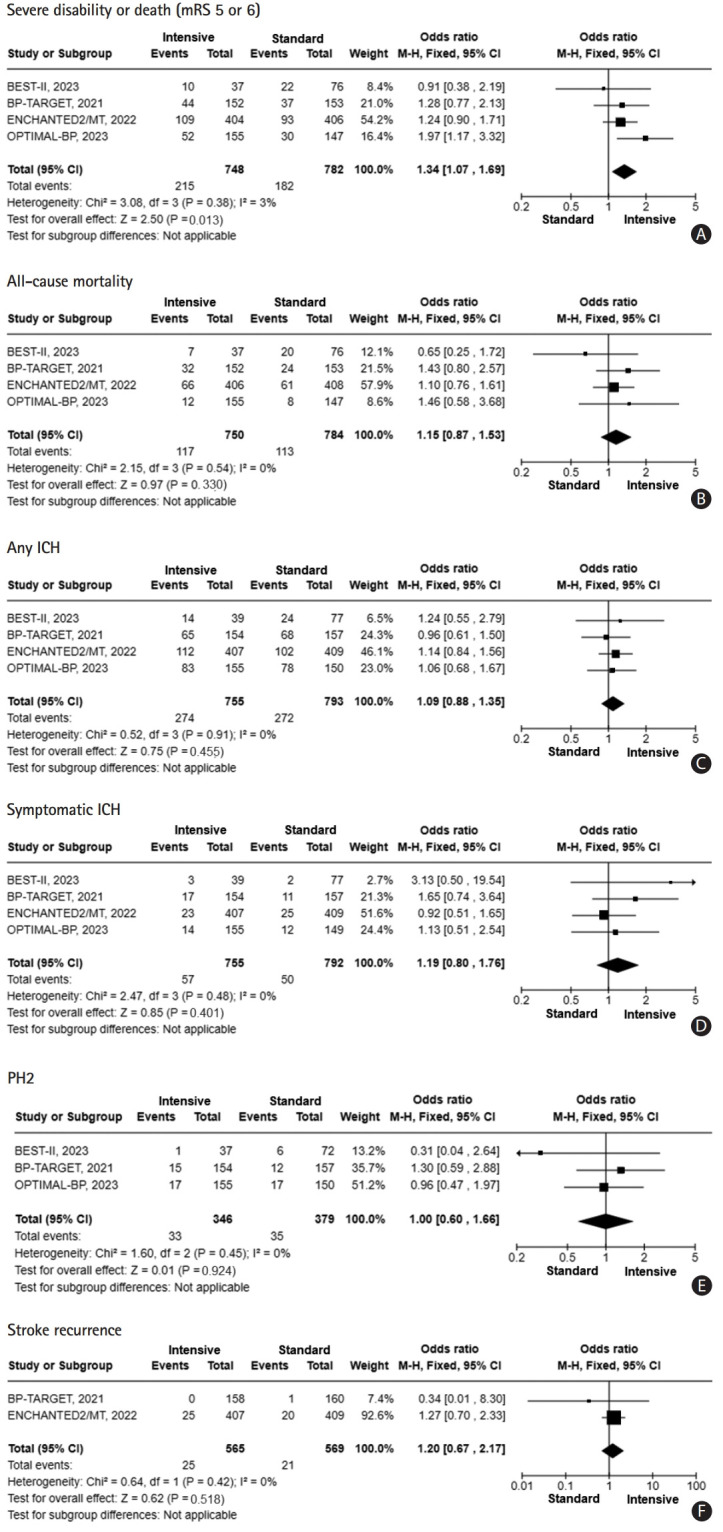
Results: Four RCTs involving 1,559 participants were included. Regarding efficacy outcomes, intensive BP control was associated with a lower likelihood of functional independence (OR: 0.68; 95% CI: 0.51-0.91 for modified Rankin Scale [mRS] ≤2) and walking without assistance (OR: 0.65; 95% CI: 0.53-0.81 for mRS ≤3). For safety outcomes, consistent with the efficacy findings, intensive BP control was significantly associated with severe disability or death (mRS 5 or 6) (OR: 1.34; 95% CI: 1.07-1.69). However, there were no significant differences including all-cause mortality, any intracerebral hemorrhage (ICH), symptomatic ICH, parenchymal hematoma type 2, and stroke recurrence.
Conclusion: While all four RCTs were conducted to demonstrate the superiority of intensive BP control over standard BP control, standard BP control may be beneficial for the outcome after EVT for AIS with LVO without increasing adverse safety outcomes. Caution should be needed with the application of intensive BP control during the 24 hours following successful recanalization after EVT.
Journal of StrokeCLINICAL NEUROLOGYPERIPHERAL VASCULAR DISE-PERIPHERAL VASCULAR DISEASE
CiteScore
11.00
自引率
3.70%
发文量
52
审稿时长
12 weeks
期刊介绍:
The Journal of Stroke (JoS) is a peer-reviewed publication that focuses on clinical and basic investigation of cerebral circulation and associated diseases in stroke-related fields. Its aim is to enhance patient management, education, clinical or experimental research, and professionalism. The journal covers various areas of stroke research, including pathophysiology, risk factors, symptomatology, imaging, treatment, and rehabilitation. Basic science research is included when it provides clinically relevant information. The JoS is particularly interested in studies that highlight characteristics of stroke in the Asian population, as they are underrepresented in the literature.
The JoS had an impact factor of 8.2 in 2022 and aims to provide high-quality research papers to readers while maintaining a strong reputation. It is published three times a year, on the last day of January, May, and September. The online version of the journal is considered the main version as it includes all available content. Supplementary issues are occasionally published.
The journal is indexed in various databases, including SCI(E), Pubmed, PubMed Central, Scopus, KoreaMed, Komci, Synapse, Science Central, Google Scholar, and DOI/Crossref. It is also the official journal of the Korean Stroke Society since 1999, with the abbreviated title J Stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


