Emily Sangillo, Neena Jube-Desai, Dina El-Metwally, Colleen Hughes Driscoll
{"title":"临床决策支持警报对新生儿重症监护室知情同意文件的影响。","authors":"Emily Sangillo, Neena Jube-Desai, Dina El-Metwally, Colleen Hughes Driscoll","doi":"10.1097/pq9.0000000000000713","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Informed consent is necessary to preserve patient autonomy and shared decision-making, yet compliant consent documentation is suboptimal in the intensive care unit (ICU). We aimed to increase compliance with bundled consent documentation, which provides consent for a predefined set of common procedures in the neonatal ICU from 0% to 50% over 1 year.</p><p><strong>Methods: </strong>We used the Plan-Do-Study-Act model for quality improvement. Interventions included education and performance awareness, delineation of the preferred consenting process, consent form revision, overlay tool creation, and clinical decision support (CDS) alert use within the electronic health record. Monthly audits categorized consent forms as missing, present but noncompliant, or compliant. We analyzed consent compliance on a run chart using standard run chart interpretation rules and obtained feedback on the CDS as a countermeasure.</p><p><strong>Results: </strong>We conducted 564 audits over 37 months. Overall, median consent compliance increased from 0% to 86.6%. Upon initiating the CDS alert, we observed the highest monthly compliance of 93.3%, followed by a decrease to 33.3% with an inadvertent discontinuation of the CDS. Compliance subsequently increased to 73.3% after the restoration of the alert. We created a consultant opt-out selection to address negative feedback associated with CDS. There were no missing consent forms within the last 7 months of monitoring.</p><p><strong>Conclusions: </strong>A multi-faceted approach led to sustained improvement in bundled consent documentation compliance in our neonatal intensive care unit, with the direct contribution of the CDS observed. A CDS intervention directed at the informed consenting process may similarly benefit other ICUs.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 1","pages":"e713"},"PeriodicalIF":1.1000,"publicationDate":"2024-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10843373/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of a Clinical Decision Support Alert on Informed Consent Documentation in the Neonatal Intensive Care Unit.\",\"authors\":\"Emily Sangillo, Neena Jube-Desai, Dina El-Metwally, Colleen Hughes Driscoll\",\"doi\":\"10.1097/pq9.0000000000000713\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Informed consent is necessary to preserve patient autonomy and shared decision-making, yet compliant consent documentation is suboptimal in the intensive care unit (ICU). We aimed to increase compliance with bundled consent documentation, which provides consent for a predefined set of common procedures in the neonatal ICU from 0% to 50% over 1 year.</p><p><strong>Methods: </strong>We used the Plan-Do-Study-Act model for quality improvement. Interventions included education and performance awareness, delineation of the preferred consenting process, consent form revision, overlay tool creation, and clinical decision support (CDS) alert use within the electronic health record. Monthly audits categorized consent forms as missing, present but noncompliant, or compliant. We analyzed consent compliance on a run chart using standard run chart interpretation rules and obtained feedback on the CDS as a countermeasure.</p><p><strong>Results: </strong>We conducted 564 audits over 37 months. Overall, median consent compliance increased from 0% to 86.6%. Upon initiating the CDS alert, we observed the highest monthly compliance of 93.3%, followed by a decrease to 33.3% with an inadvertent discontinuation of the CDS. Compliance subsequently increased to 73.3% after the restoration of the alert. We created a consultant opt-out selection to address negative feedback associated with CDS. There were no missing consent forms within the last 7 months of monitoring.</p><p><strong>Conclusions: </strong>A multi-faceted approach led to sustained improvement in bundled consent documentation compliance in our neonatal intensive care unit, with the direct contribution of the CDS observed. A CDS intervention directed at the informed consenting process may similarly benefit other ICUs.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"9 1\",\"pages\":\"e713\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-02-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10843373/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000713\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000713","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Impact of a Clinical Decision Support Alert on Informed Consent Documentation in the Neonatal Intensive Care Unit.
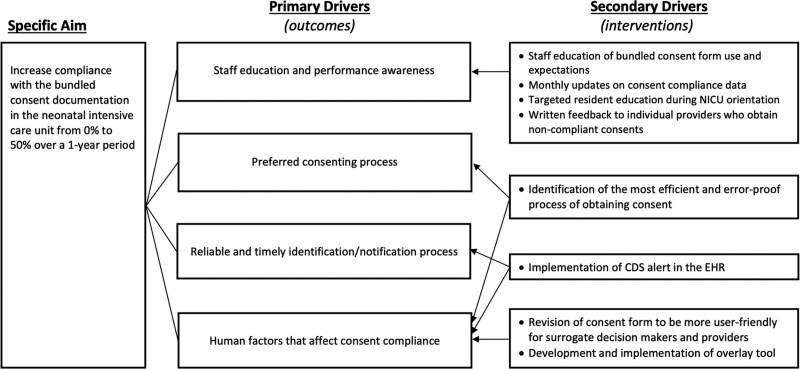
Background: Informed consent is necessary to preserve patient autonomy and shared decision-making, yet compliant consent documentation is suboptimal in the intensive care unit (ICU). We aimed to increase compliance with bundled consent documentation, which provides consent for a predefined set of common procedures in the neonatal ICU from 0% to 50% over 1 year.
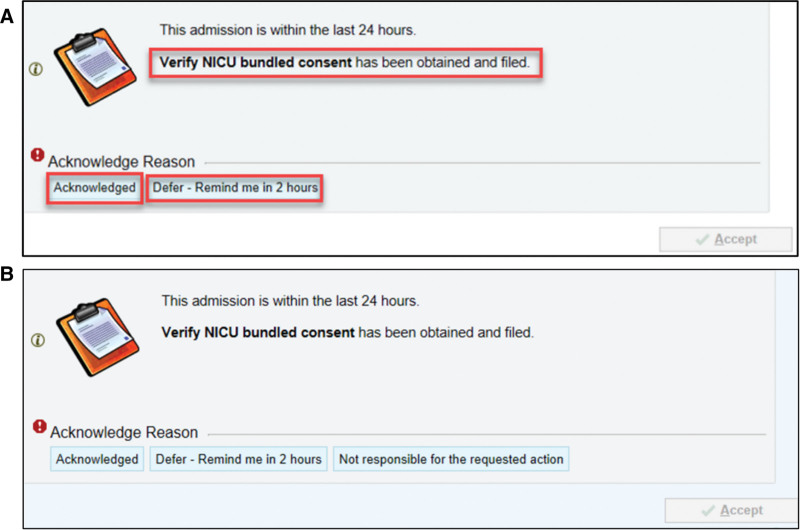
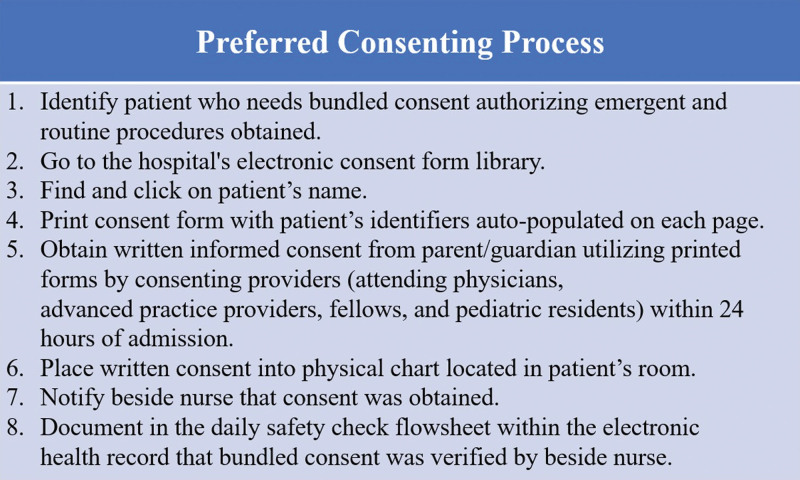
Methods: We used the Plan-Do-Study-Act model for quality improvement. Interventions included education and performance awareness, delineation of the preferred consenting process, consent form revision, overlay tool creation, and clinical decision support (CDS) alert use within the electronic health record. Monthly audits categorized consent forms as missing, present but noncompliant, or compliant. We analyzed consent compliance on a run chart using standard run chart interpretation rules and obtained feedback on the CDS as a countermeasure.
Results: We conducted 564 audits over 37 months. Overall, median consent compliance increased from 0% to 86.6%. Upon initiating the CDS alert, we observed the highest monthly compliance of 93.3%, followed by a decrease to 33.3% with an inadvertent discontinuation of the CDS. Compliance subsequently increased to 73.3% after the restoration of the alert. We created a consultant opt-out selection to address negative feedback associated with CDS. There were no missing consent forms within the last 7 months of monitoring.
Conclusions: A multi-faceted approach led to sustained improvement in bundled consent documentation compliance in our neonatal intensive care unit, with the direct contribution of the CDS observed. A CDS intervention directed at the informed consenting process may similarly benefit other ICUs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


