Andrew J Armstrong, Ravit Geva, Hyun Cheol Chung, Charlotte Lemech, Wilson H Miller, Aaron R Hansen, Jong-Seok Lee, Frank Tsai, Benjamin J Solomon, Tae Min Kim, Christian Rolfo, Vincent Giranda, Yixin Ren, Fang Liu, Bhargava Kandala, Tomoko Freshwater, Judy S Wang
{"title":"CXCR2拮抗剂纳瓦利辛与pembrolizumab联合治疗部分晚期实体瘤:2期随机试验。","authors":"Andrew J Armstrong, Ravit Geva, Hyun Cheol Chung, Charlotte Lemech, Wilson H Miller, Aaron R Hansen, Jong-Seok Lee, Frank Tsai, Benjamin J Solomon, Tae Min Kim, Christian Rolfo, Vincent Giranda, Yixin Ren, Fang Liu, Bhargava Kandala, Tomoko Freshwater, Judy S Wang","doi":"10.1007/s10637-023-01410-2","DOIUrl":null,"url":null,"abstract":"<p><p>C-X-C motif chemokine receptor 2 (CXCR2) has a role in tumor progression, lineage plasticity, and reduction of immune checkpoint inhibitor efficacy. Preclinical evidence suggests potential benefit of CXCR2 inhibition in multiple solid tumors. In this phase 2 study (NCT03473925), adults with previously treated advanced or metastatic castration-resistant prostate cancer (CRPC), microsatellite-stable colorectal cancer (MSS CRC), or non-small-cell lung cancer (NSCLC) were randomized 1:1 to the CXCR2 antagonist navarixin 30 or 100 mg orally once daily plus pembrolizumab 200 mg intravenously every 3 weeks up to 35 cycles. Primary endpoints were investigator-assessed objective response rate (RECIST v1.1) and safety. Of 105 patients (CRPC, n=40; MSS CRC, n=40; NSCLC, n=25), 3 had a partial response (2 CRPC, 1 MSS CRC) for ORRs of 5%, 2.5%, and 0%, respectively. Median progression-free survival was 1.8-2.4 months without evidence of a dose-response relationship, and the study was closed at a prespecified interim analysis for lack of efficacy. Dose-limiting toxicities occurred in 2/48 patients (4%) receiving navarixin 30 mg and 3/48 (6%) receiving navarixin 100 mg; events included grade 4 neutropenia and grade 3 transaminase elevation, hepatitis, and pneumonitis. Treatment-related adverse events occurred in 70/105 patients (67%) and led to treatment discontinuation in 7/105 (7%). Maximal reductions from baseline in absolute neutrophil count were 44.5%-48.2% (cycle 1) and 37.5%-44.2% (cycle 2) and occurred within 6-12 hours postdose in both groups. Navarixin plus pembrolizumab did not demonstrate sufficient efficacy in this study. Safety and tolerability of the combination were manageable. (Trial registration: ClinicalTrials.gov , NCT03473925).</p>","PeriodicalId":14513,"journal":{"name":"Investigational New Drugs","volume":" ","pages":"145-159"},"PeriodicalIF":3.0000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11076327/pdf/","citationCount":"0","resultStr":"{\"title\":\"CXCR2 antagonist navarixin in combination with pembrolizumab in select advanced solid tumors: a phase 2 randomized trial.\",\"authors\":\"Andrew J Armstrong, Ravit Geva, Hyun Cheol Chung, Charlotte Lemech, Wilson H Miller, Aaron R Hansen, Jong-Seok Lee, Frank Tsai, Benjamin J Solomon, Tae Min Kim, Christian Rolfo, Vincent Giranda, Yixin Ren, Fang Liu, Bhargava Kandala, Tomoko Freshwater, Judy S Wang\",\"doi\":\"10.1007/s10637-023-01410-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>C-X-C motif chemokine receptor 2 (CXCR2) has a role in tumor progression, lineage plasticity, and reduction of immune checkpoint inhibitor efficacy. Preclinical evidence suggests potential benefit of CXCR2 inhibition in multiple solid tumors. In this phase 2 study (NCT03473925), adults with previously treated advanced or metastatic castration-resistant prostate cancer (CRPC), microsatellite-stable colorectal cancer (MSS CRC), or non-small-cell lung cancer (NSCLC) were randomized 1:1 to the CXCR2 antagonist navarixin 30 or 100 mg orally once daily plus pembrolizumab 200 mg intravenously every 3 weeks up to 35 cycles. Primary endpoints were investigator-assessed objective response rate (RECIST v1.1) and safety. Of 105 patients (CRPC, n=40; MSS CRC, n=40; NSCLC, n=25), 3 had a partial response (2 CRPC, 1 MSS CRC) for ORRs of 5%, 2.5%, and 0%, respectively. Median progression-free survival was 1.8-2.4 months without evidence of a dose-response relationship, and the study was closed at a prespecified interim analysis for lack of efficacy. Dose-limiting toxicities occurred in 2/48 patients (4%) receiving navarixin 30 mg and 3/48 (6%) receiving navarixin 100 mg; events included grade 4 neutropenia and grade 3 transaminase elevation, hepatitis, and pneumonitis. Treatment-related adverse events occurred in 70/105 patients (67%) and led to treatment discontinuation in 7/105 (7%). Maximal reductions from baseline in absolute neutrophil count were 44.5%-48.2% (cycle 1) and 37.5%-44.2% (cycle 2) and occurred within 6-12 hours postdose in both groups. Navarixin plus pembrolizumab did not demonstrate sufficient efficacy in this study. Safety and tolerability of the combination were manageable. (Trial registration: ClinicalTrials.gov , NCT03473925).</p>\",\"PeriodicalId\":14513,\"journal\":{\"name\":\"Investigational New Drugs\",\"volume\":\" \",\"pages\":\"145-159\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11076327/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Investigational New Drugs\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10637-023-01410-2\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Investigational New Drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10637-023-01410-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
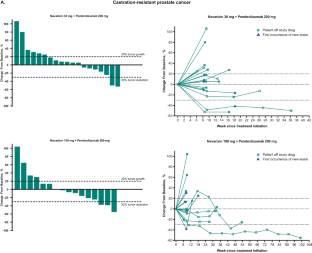
CXCR2 antagonist navarixin in combination with pembrolizumab in select advanced solid tumors: a phase 2 randomized trial.
C-X-C motif chemokine receptor 2 (CXCR2) has a role in tumor progression, lineage plasticity, and reduction of immune checkpoint inhibitor efficacy. Preclinical evidence suggests potential benefit of CXCR2 inhibition in multiple solid tumors. In this phase 2 study (NCT03473925), adults with previously treated advanced or metastatic castration-resistant prostate cancer (CRPC), microsatellite-stable colorectal cancer (MSS CRC), or non-small-cell lung cancer (NSCLC) were randomized 1:1 to the CXCR2 antagonist navarixin 30 or 100 mg orally once daily plus pembrolizumab 200 mg intravenously every 3 weeks up to 35 cycles. Primary endpoints were investigator-assessed objective response rate (RECIST v1.1) and safety. Of 105 patients (CRPC, n=40; MSS CRC, n=40; NSCLC, n=25), 3 had a partial response (2 CRPC, 1 MSS CRC) for ORRs of 5%, 2.5%, and 0%, respectively. Median progression-free survival was 1.8-2.4 months without evidence of a dose-response relationship, and the study was closed at a prespecified interim analysis for lack of efficacy. Dose-limiting toxicities occurred in 2/48 patients (4%) receiving navarixin 30 mg and 3/48 (6%) receiving navarixin 100 mg; events included grade 4 neutropenia and grade 3 transaminase elevation, hepatitis, and pneumonitis. Treatment-related adverse events occurred in 70/105 patients (67%) and led to treatment discontinuation in 7/105 (7%). Maximal reductions from baseline in absolute neutrophil count were 44.5%-48.2% (cycle 1) and 37.5%-44.2% (cycle 2) and occurred within 6-12 hours postdose in both groups. Navarixin plus pembrolizumab did not demonstrate sufficient efficacy in this study. Safety and tolerability of the combination were manageable. (Trial registration: ClinicalTrials.gov , NCT03473925).
期刊介绍:
The development of new anticancer agents is one of the most rapidly changing aspects of cancer research. Investigational New Drugs provides a forum for the rapid dissemination of information on new anticancer agents. The papers published are of interest to the medical chemist, toxicologist, pharmacist, pharmacologist, biostatistician and clinical oncologist. Investigational New Drugs provides the fastest possible publication of new discoveries and results for the whole community of scientists developing anticancer agents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


