Yan Peng, Wei Zhao, Dachuan Zhang, Xie Gao, Yongqiang Shi, Qing Li, Jian Wang
{"title":"一名颅内肿块反复发作的 24 岁女性。","authors":"Yan Peng, Wei Zhao, Dachuan Zhang, Xie Gao, Yongqiang Shi, Qing Li, Jian Wang","doi":"10.1111/bpa.13242","DOIUrl":null,"url":null,"abstract":"<p>A 24-year-old woman presented with headache, dizziness, and tinnitus that had lasted for 3 months. Pre-operative magnetic resonance imaging (MRI) demonstrated a 6 × 4.9 × 4.3 cm well-circumscribed mass located in the right frontal lobe adjacent to the cerebral falx. The mass showed heterogeneous signal intensity and both solid and cystic components with perilesional brain edema on T1-weighted (Figure 1A) and T2-weighted images. Microsurgical tumor resection was performed. During the operation, it was found that the tumor originated from the falx and had infiltrated the opposite side. Gross total resection of the tumor was achieved with the adherent falx. The patient received no adjuvant treatment after the operation and had local recurrence 26 months after surgery, marked by the presence of headache. MRI demonstrated a 4.5 × 3.0 × 2.9 cm cystic-solid mass at the local recurrence (Figure 1B). The patient underwent gross total resection again and had a disease-free survival time of 14 months.</p><p>Histopathological examination revealed similar morphological features in both primary and recurrent tumors (Box 1). A fibrous pseudocapsule was present at the periphery of both tumors, which showed solid tumor cell nodules. A dense lymphoplasmacytic infiltrate with lymphoid follicles was present along the pseudocapsule and the periphery of the nodules (Figure 2A), which led to our first consideration of angiomatoid fibrous histiocytoma (AFH). Blood-filled pseudoangiomatoid cystic spaces and intratumor hemorrhage with hemosiderin were identified. Tumor cell morphology mainly included epithelioid, rhabdoid (Figure 2B), oval, and spindle morphology. Epithelioid cells embedded in a dense sclerotic stroma were seen (Figure 2C). The tumor cells had indistinct cell borders and inconspicuous nucleoli. Mitotic activity was low. Immunohistochemistry, the tumor cells were diffusely positive for desmin (Figure 2D) and CD99, and some were positive for EMA (Figure 2E) and MUC4. Few cells presented weak expression of ALK. The tumor cells were negative for S100, CD34, CD31, STAT6, HMB45, CD21, CD68, Synaptophysin, Chromogranin, WT1. The Ki-67 index was 5%. Next-generation sequencing (NGS) revealed that the tumor harbored exon 7 of the FUS gene and exon 6 of the CREM gene fusion (Figure 2F).</p><p>Intracranial mesenchymal tumor, <i>FET::CREB</i> fusion-positive.</p><p>FET family (EWSR1 and FUS) fusions with CREB family (CREB1, CREM, and ATF1) are found in a wide variety of tumor entities. Kao et al [<span>1</span>] first reported the occurrence of a unique myxoid mesenchymal tumor with <i>EWSR1</i> fusions with <i>CREB</i> family members in young patients with intracranial predilection in 2017. Previous studies speculated that these tumors may represent a myxoid variant of AFH occurring intracranially or a novel intracranial myxoid mesenchymal tumor (IMMT). Sloan et al. [<span>2</span>] studied the largest numbers of these tumors, reviewed previously reported cases, and unified the diagnosis for the spectrum of these tumors as Intracranial mesenchymal tumor with <i>FET::CREB</i> fusion. Intracranial mesenchymal tumor, <i>FET::CREB</i> fusion-positive has been added as a newly recognized provisional entity in the section of Mesenchymal, Non-Meningothelial Tumors in the 2021 fifth edition of the WHO Classification of Tumors of the Central Nervous System (CNS) [<span>3</span>]. Of all these intracranial mesenchymal tumors reported with <i>FET::CREB</i> fusions, most tumors have <i>EWSR1::ATF1</i> fusion, <i>EWSR1::CREB1</i> fusion, <i>EWSR1::CREM</i> fusion, and only one case has <i>FUS::CREM</i> fusion [<span>2</span>]. Here, we report another case of intracranial mesenchymal tumor with <i>FUS::CREM</i> fusion in an adult woman.</p><p>The previously reported case occurred in a four-year-old girl, with location at the cerebral convexity. The radiological characteristics of both cases demonstrate well circumscribed enhancing masses with both solid and cystic components, surrounded by the peritumoral edema. Both cases show histopathological features including epithelioid and rhabdoid cell morphology, collagenous stroma with dense intercellular matrix, dense lymphoplasmacytic cuffing at the tumor periphery, and intratumor hemorrhage with hemosiderin or hematoidin, with no mucin-rich stroma or necrosis. The tumor cells in both cases are positive for desmin, CD99, EMA, and negative for S100 and HMB45. The previously reported case demonstrates striking cytologic atypia and mitotic activity, with no pseudoangiomatoid vasculature, no spindle cell morphology, and positivity for CD68, in contrast to the current case. Some tumor cells are positive for MUC4 in the current case, raising the differential diagnosis with low-grade fibromyxoid sarcoma (LGFMS) or sclerosing epithelioid fibrosarcoma (SEF), tumors which are generally negative for desmin and harbor <i>FUS/EWSR1::CREB3L1/CREB3L2</i> fusion. The expression of EMA may cause a misdiagnosis of meningioma, but these tumors are positive for desmin and negative for SSTR2A immunohistochemically, and lack meningioma-associated mutations in NF2.</p><p>In terms of clinical outcomes, the previously reported patient had two local recurrences (9 months and 13 months), and was still alive with a disease-free at 36 months. Intracranial mesenchymal tumor, <i>FET::CREB</i> fusion-positive occurs with a female predominance and a wide age range, and shares the common histological features that were previously described in AFH and IMMT. Although there is some evidence that these tumors have a propensity for local recurrence and occasional metastasis, the WHO does not provide a definite grading. Larger studies are needed to explore these rare tumors.</p><p>All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Yan Peng, Wei Zhao, Dachuan Zhang, Xie Gao, and Yongqiang Shi. The first draft of the manuscript was written by Yan Peng. Qing Li and Jian Wang gave final approval.</p><p>No funding was received for conducting this study.</p><p>The authors declare no conflict of interest.</p><p>The study was approved by the ethics committee of The Third Affiliated Hospital of Soochow University, Changzhou First People's Hospital, Changzhou, China.</p>","PeriodicalId":9290,"journal":{"name":"Brain Pathology","volume":"34 2","pages":""},"PeriodicalIF":5.8000,"publicationDate":"2024-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bpa.13242","citationCount":"0","resultStr":"{\"title\":\"A 24-year-old woman with a recurrent intracranial mass\",\"authors\":\"Yan Peng, Wei Zhao, Dachuan Zhang, Xie Gao, Yongqiang Shi, Qing Li, Jian Wang\",\"doi\":\"10.1111/bpa.13242\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 24-year-old woman presented with headache, dizziness, and tinnitus that had lasted for 3 months. Pre-operative magnetic resonance imaging (MRI) demonstrated a 6 × 4.9 × 4.3 cm well-circumscribed mass located in the right frontal lobe adjacent to the cerebral falx. The mass showed heterogeneous signal intensity and both solid and cystic components with perilesional brain edema on T1-weighted (Figure 1A) and T2-weighted images. Microsurgical tumor resection was performed. During the operation, it was found that the tumor originated from the falx and had infiltrated the opposite side. Gross total resection of the tumor was achieved with the adherent falx. The patient received no adjuvant treatment after the operation and had local recurrence 26 months after surgery, marked by the presence of headache. MRI demonstrated a 4.5 × 3.0 × 2.9 cm cystic-solid mass at the local recurrence (Figure 1B). The patient underwent gross total resection again and had a disease-free survival time of 14 months.</p><p>Histopathological examination revealed similar morphological features in both primary and recurrent tumors (Box 1). A fibrous pseudocapsule was present at the periphery of both tumors, which showed solid tumor cell nodules. A dense lymphoplasmacytic infiltrate with lymphoid follicles was present along the pseudocapsule and the periphery of the nodules (Figure 2A), which led to our first consideration of angiomatoid fibrous histiocytoma (AFH). Blood-filled pseudoangiomatoid cystic spaces and intratumor hemorrhage with hemosiderin were identified. Tumor cell morphology mainly included epithelioid, rhabdoid (Figure 2B), oval, and spindle morphology. Epithelioid cells embedded in a dense sclerotic stroma were seen (Figure 2C). The tumor cells had indistinct cell borders and inconspicuous nucleoli. Mitotic activity was low. Immunohistochemistry, the tumor cells were diffusely positive for desmin (Figure 2D) and CD99, and some were positive for EMA (Figure 2E) and MUC4. Few cells presented weak expression of ALK. The tumor cells were negative for S100, CD34, CD31, STAT6, HMB45, CD21, CD68, Synaptophysin, Chromogranin, WT1. The Ki-67 index was 5%. Next-generation sequencing (NGS) revealed that the tumor harbored exon 7 of the FUS gene and exon 6 of the CREM gene fusion (Figure 2F).</p><p>Intracranial mesenchymal tumor, <i>FET::CREB</i> fusion-positive.</p><p>FET family (EWSR1 and FUS) fusions with CREB family (CREB1, CREM, and ATF1) are found in a wide variety of tumor entities. Kao et al [<span>1</span>] first reported the occurrence of a unique myxoid mesenchymal tumor with <i>EWSR1</i> fusions with <i>CREB</i> family members in young patients with intracranial predilection in 2017. Previous studies speculated that these tumors may represent a myxoid variant of AFH occurring intracranially or a novel intracranial myxoid mesenchymal tumor (IMMT). Sloan et al. [<span>2</span>] studied the largest numbers of these tumors, reviewed previously reported cases, and unified the diagnosis for the spectrum of these tumors as Intracranial mesenchymal tumor with <i>FET::CREB</i> fusion. Intracranial mesenchymal tumor, <i>FET::CREB</i> fusion-positive has been added as a newly recognized provisional entity in the section of Mesenchymal, Non-Meningothelial Tumors in the 2021 fifth edition of the WHO Classification of Tumors of the Central Nervous System (CNS) [<span>3</span>]. Of all these intracranial mesenchymal tumors reported with <i>FET::CREB</i> fusions, most tumors have <i>EWSR1::ATF1</i> fusion, <i>EWSR1::CREB1</i> fusion, <i>EWSR1::CREM</i> fusion, and only one case has <i>FUS::CREM</i> fusion [<span>2</span>]. Here, we report another case of intracranial mesenchymal tumor with <i>FUS::CREM</i> fusion in an adult woman.</p><p>The previously reported case occurred in a four-year-old girl, with location at the cerebral convexity. The radiological characteristics of both cases demonstrate well circumscribed enhancing masses with both solid and cystic components, surrounded by the peritumoral edema. Both cases show histopathological features including epithelioid and rhabdoid cell morphology, collagenous stroma with dense intercellular matrix, dense lymphoplasmacytic cuffing at the tumor periphery, and intratumor hemorrhage with hemosiderin or hematoidin, with no mucin-rich stroma or necrosis. The tumor cells in both cases are positive for desmin, CD99, EMA, and negative for S100 and HMB45. The previously reported case demonstrates striking cytologic atypia and mitotic activity, with no pseudoangiomatoid vasculature, no spindle cell morphology, and positivity for CD68, in contrast to the current case. Some tumor cells are positive for MUC4 in the current case, raising the differential diagnosis with low-grade fibromyxoid sarcoma (LGFMS) or sclerosing epithelioid fibrosarcoma (SEF), tumors which are generally negative for desmin and harbor <i>FUS/EWSR1::CREB3L1/CREB3L2</i> fusion. The expression of EMA may cause a misdiagnosis of meningioma, but these tumors are positive for desmin and negative for SSTR2A immunohistochemically, and lack meningioma-associated mutations in NF2.</p><p>In terms of clinical outcomes, the previously reported patient had two local recurrences (9 months and 13 months), and was still alive with a disease-free at 36 months. Intracranial mesenchymal tumor, <i>FET::CREB</i> fusion-positive occurs with a female predominance and a wide age range, and shares the common histological features that were previously described in AFH and IMMT. Although there is some evidence that these tumors have a propensity for local recurrence and occasional metastasis, the WHO does not provide a definite grading. Larger studies are needed to explore these rare tumors.</p><p>All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Yan Peng, Wei Zhao, Dachuan Zhang, Xie Gao, and Yongqiang Shi. The first draft of the manuscript was written by Yan Peng. Qing Li and Jian Wang gave final approval.</p><p>No funding was received for conducting this study.</p><p>The authors declare no conflict of interest.</p><p>The study was approved by the ethics committee of The Third Affiliated Hospital of Soochow University, Changzhou First People's Hospital, Changzhou, China.</p>\",\"PeriodicalId\":9290,\"journal\":{\"name\":\"Brain Pathology\",\"volume\":\"34 2\",\"pages\":\"\"},\"PeriodicalIF\":5.8000,\"publicationDate\":\"2024-02-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bpa.13242\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brain Pathology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/bpa.13242\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Pathology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bpa.13242","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
A 24-year-old woman with a recurrent intracranial mass
A 24-year-old woman presented with headache, dizziness, and tinnitus that had lasted for 3 months. Pre-operative magnetic resonance imaging (MRI) demonstrated a 6 × 4.9 × 4.3 cm well-circumscribed mass located in the right frontal lobe adjacent to the cerebral falx. The mass showed heterogeneous signal intensity and both solid and cystic components with perilesional brain edema on T1-weighted (Figure 1A) and T2-weighted images. Microsurgical tumor resection was performed. During the operation, it was found that the tumor originated from the falx and had infiltrated the opposite side. Gross total resection of the tumor was achieved with the adherent falx. The patient received no adjuvant treatment after the operation and had local recurrence 26 months after surgery, marked by the presence of headache. MRI demonstrated a 4.5 × 3.0 × 2.9 cm cystic-solid mass at the local recurrence (Figure 1B). The patient underwent gross total resection again and had a disease-free survival time of 14 months.
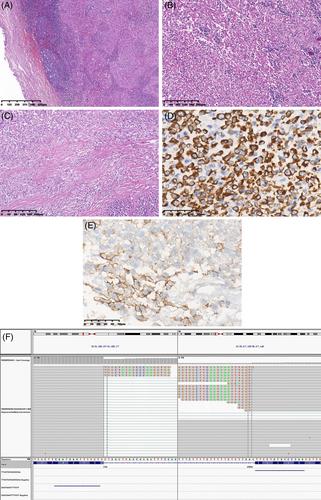
Histopathological examination revealed similar morphological features in both primary and recurrent tumors (Box 1). A fibrous pseudocapsule was present at the periphery of both tumors, which showed solid tumor cell nodules. A dense lymphoplasmacytic infiltrate with lymphoid follicles was present along the pseudocapsule and the periphery of the nodules (Figure 2A), which led to our first consideration of angiomatoid fibrous histiocytoma (AFH). Blood-filled pseudoangiomatoid cystic spaces and intratumor hemorrhage with hemosiderin were identified. Tumor cell morphology mainly included epithelioid, rhabdoid (Figure 2B), oval, and spindle morphology. Epithelioid cells embedded in a dense sclerotic stroma were seen (Figure 2C). The tumor cells had indistinct cell borders and inconspicuous nucleoli. Mitotic activity was low. Immunohistochemistry, the tumor cells were diffusely positive for desmin (Figure 2D) and CD99, and some were positive for EMA (Figure 2E) and MUC4. Few cells presented weak expression of ALK. The tumor cells were negative for S100, CD34, CD31, STAT6, HMB45, CD21, CD68, Synaptophysin, Chromogranin, WT1. The Ki-67 index was 5%. Next-generation sequencing (NGS) revealed that the tumor harbored exon 7 of the FUS gene and exon 6 of the CREM gene fusion (Figure 2F).
FET family (EWSR1 and FUS) fusions with CREB family (CREB1, CREM, and ATF1) are found in a wide variety of tumor entities. Kao et al [1] first reported the occurrence of a unique myxoid mesenchymal tumor with EWSR1 fusions with CREB family members in young patients with intracranial predilection in 2017. Previous studies speculated that these tumors may represent a myxoid variant of AFH occurring intracranially or a novel intracranial myxoid mesenchymal tumor (IMMT). Sloan et al. [2] studied the largest numbers of these tumors, reviewed previously reported cases, and unified the diagnosis for the spectrum of these tumors as Intracranial mesenchymal tumor with FET::CREB fusion. Intracranial mesenchymal tumor, FET::CREB fusion-positive has been added as a newly recognized provisional entity in the section of Mesenchymal, Non-Meningothelial Tumors in the 2021 fifth edition of the WHO Classification of Tumors of the Central Nervous System (CNS) [3]. Of all these intracranial mesenchymal tumors reported with FET::CREB fusions, most tumors have EWSR1::ATF1 fusion, EWSR1::CREB1 fusion, EWSR1::CREM fusion, and only one case has FUS::CREM fusion [2]. Here, we report another case of intracranial mesenchymal tumor with FUS::CREM fusion in an adult woman.
The previously reported case occurred in a four-year-old girl, with location at the cerebral convexity. The radiological characteristics of both cases demonstrate well circumscribed enhancing masses with both solid and cystic components, surrounded by the peritumoral edema. Both cases show histopathological features including epithelioid and rhabdoid cell morphology, collagenous stroma with dense intercellular matrix, dense lymphoplasmacytic cuffing at the tumor periphery, and intratumor hemorrhage with hemosiderin or hematoidin, with no mucin-rich stroma or necrosis. The tumor cells in both cases are positive for desmin, CD99, EMA, and negative for S100 and HMB45. The previously reported case demonstrates striking cytologic atypia and mitotic activity, with no pseudoangiomatoid vasculature, no spindle cell morphology, and positivity for CD68, in contrast to the current case. Some tumor cells are positive for MUC4 in the current case, raising the differential diagnosis with low-grade fibromyxoid sarcoma (LGFMS) or sclerosing epithelioid fibrosarcoma (SEF), tumors which are generally negative for desmin and harbor FUS/EWSR1::CREB3L1/CREB3L2 fusion. The expression of EMA may cause a misdiagnosis of meningioma, but these tumors are positive for desmin and negative for SSTR2A immunohistochemically, and lack meningioma-associated mutations in NF2.
In terms of clinical outcomes, the previously reported patient had two local recurrences (9 months and 13 months), and was still alive with a disease-free at 36 months. Intracranial mesenchymal tumor, FET::CREB fusion-positive occurs with a female predominance and a wide age range, and shares the common histological features that were previously described in AFH and IMMT. Although there is some evidence that these tumors have a propensity for local recurrence and occasional metastasis, the WHO does not provide a definite grading. Larger studies are needed to explore these rare tumors.
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Yan Peng, Wei Zhao, Dachuan Zhang, Xie Gao, and Yongqiang Shi. The first draft of the manuscript was written by Yan Peng. Qing Li and Jian Wang gave final approval.
No funding was received for conducting this study.
The authors declare no conflict of interest.
The study was approved by the ethics committee of The Third Affiliated Hospital of Soochow University, Changzhou First People's Hospital, Changzhou, China.
期刊介绍:
Brain Pathology is the journal of choice for biomedical scientists investigating diseases of the nervous system. The official journal of the International Society of Neuropathology, Brain Pathology is a peer-reviewed quarterly publication that includes original research, review articles and symposia focuses on the pathogenesis of neurological disease.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


